

Adverse events after colonoscopy in a randomised colorectal cancer screening trial
- PMID: 39375173
- PMCID: PMC11459295
- DOI: 10.1136/bmjgast-2024-001471
Adverse events after colonoscopy in a randomised colorectal cancer screening trial
Abstract
Objective: Colonoscopy-related adverse events increase the burden of colorectal cancer (CRC) screening. This cross-sectional study evaluates adverse events during and after colonoscopy in a large, randomised CRC screening trial in Norway comparing sigmoidoscopy to immunochemical testing for faecal blood.
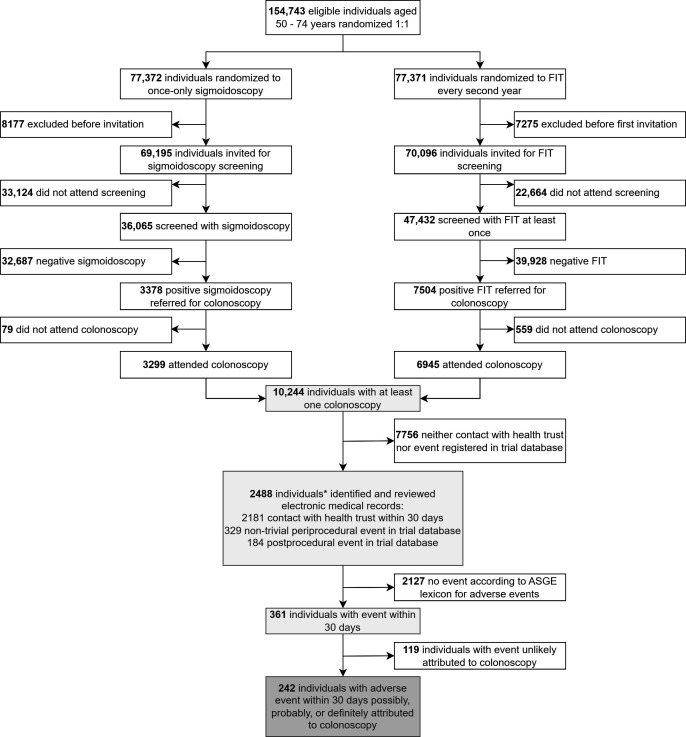
Methods: We included all individuals who underwent colonoscopy at two screening centres between 2012 and 2020. From medical records, we retrieved data on adverse events during and within 30 days after colonoscopy and classified them according to the American Society for Gastrointestinal Endoscopy lexicon for endoscopic adverse events. Multivariable logistic regression models were fitted to identify risk factors for adverse events.
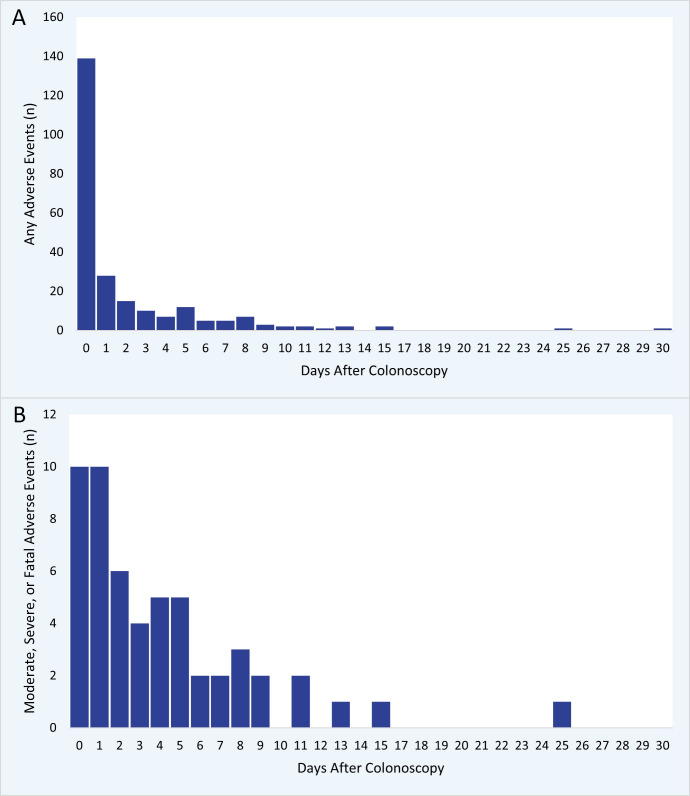
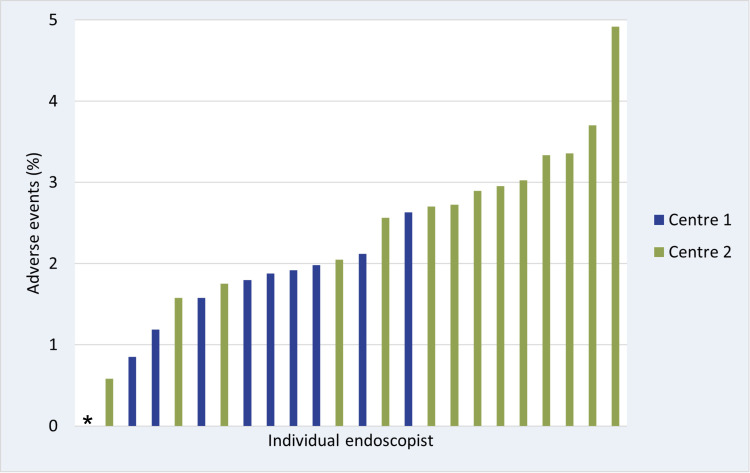
Results: Of the 10 244 included individuals, 242 (2.4%) had at least one adverse event that was possibly, probably, or definitively related to the colonoscopy. 188 (1.8%) had mild adverse events, 50 (0.49%) had moderate, 3 (0.03%) had severe, and 1 had a fatal adverse event. The most frequent adverse events were lower gastrointestinal bleeding (0.86%), abdominal pain (0.48%), vasovagal reaction (0.39%), postpolypectomy syndrome (0.20%), and perforation (0.08%). 23 (0.22%) individuals had non-gastrointestinal adverse events. Risk factors associated with adverse events were older age, female sex, screening centre, anticoagulant therapy, number of polypectomies, size of lesion removed, presence of proximal lesion, and adenocarcinoma. Adverse event rates per endoscopist ranged from 0% to 4.9%.
Conclusion: Adverse events after colonoscopy of screening positives occurred in about 2 out of 100 procedures. Three-quarters of events were mild. Awareness of risk factors may help endoscopists to mitigate the risk.
Trial registration number: NCT01538550.
Keywords: Colonoscopy; Colorectal cancer screening; Epidemiology.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: The bowel preparation used for colonoscopy was provided free of charge by Ferring Pharmaceuticals. SOF reports Chairman, The Norwegian Society of Clinical Nutrition and Metabolism; Council Member, European Society for Clinical Nutrition and Metabolism outside of the submitted work.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical