

Discontinuation of maintenance therapy in multiple myeloma guided by multimodal measurable residual disease negativity (MRD2STOP)
- PMID: 39375362
- PMCID: PMC11458825
- DOI: 10.1038/s41408-024-01156-x
Discontinuation of maintenance therapy in multiple myeloma guided by multimodal measurable residual disease negativity (MRD2STOP)
Abstract
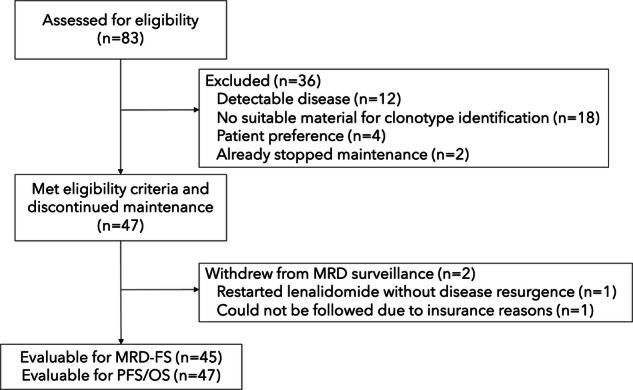
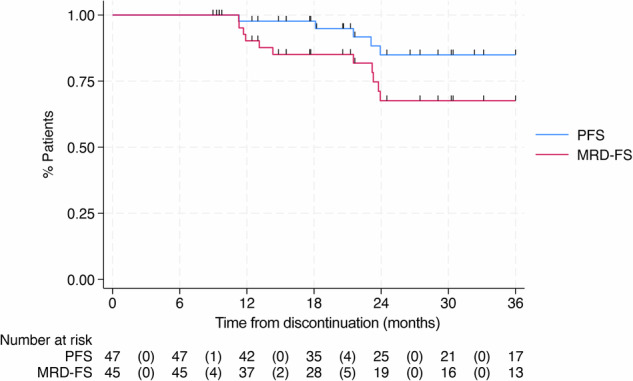
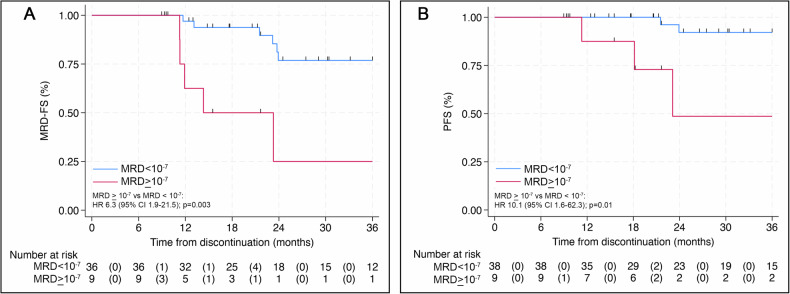
MRD2STOP is a pragmatic trial evaluating maintenance therapy cessation guided by measurable residual disease (MRD) negativity in multiple myeloma (MM). Eligible patients had previous MRD < 10-5, received ≥1 year of maintenance, and were prospectively confirmed to have undetectable disease by positron emission tomography, bone marrow (BM) flow cytometry (limit of detection [LoD] 10-5), and BM clonoSEQ (LoD 10-6). BM aspirates enriched for CD138+ cells were analyzed by clonoSEQ to achieve MRD 10-7 sensitivity. We evaluated the incidence of disease resurgence and progression-free survival (PFS), stratified by 10-7 status. Forty-seven patients discontinued maintenance after a median of 36 months. Baseline MRD ≥ 10-7 was observed in 19% (9/47). The median follow-up post-discontinuation was 30 months. Disease resurgence (MRD 10 ≥ -6) occurred in 11 patients, including 5 disease progressions. One patient died from a second cancer. The estimated 3-year cumulative incidence of disease resurgence was 20% for patients with baseline MRD < 10-7 compared to 75% for MRD ≥ 10-7 (HR 7.8, 95% CI 2.2-27.6, p = 0.001). Baseline MRD ≥ 10-7 was associated with inferior PFS compared to MRD < 10-7 (HR 10.1, 95% CI 1.6-62.3; 3-year PFS 49% vs 92%). Maintenance discontinuation in patients with MM and MRD < 10-6 led to low rates of disease resurgence. MRD < 10-7 may be a superior cessation threshold, requiring further validation.
© 2024. The Author(s).
Conflict of interest statement
B.A.D. declares consultancy for Johnson & Johnson, Sanofi, Canopy, and Cota Inc.; independent clinical trial reviewer for BMS; research funding from GSK and Amgen. A.M., J.C., K.J., A.R., Th.K., and Ta.K. have nothing to disclose. A.J.J. declares honoraria and advisory board fees from Abbvie, Amgen, Bristol-Myers Squibb/Celgene, GlaxoSmithKline, Gracell, Janssen, and Sanofi.
Figures

References
-
- Gay F, Musto P, Rota-Scalabrini D, Bertamini L, Belotti A, Galli M, et al. Carfilzomib with cyclophosphamide and dexamethasone or lenalidomide and dexamethasone plus autologous transplantation or carfilzomib plus lenalidomide and dexamethasone, followed by maintenance with carfilzomib plus lenalidomide or lenalidomide alone for patients with newly diagnosed multiple myeloma (FORTE): a randomised, open-label, phase 2 trial. Lancet Oncol. 2021;22:1705–20. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
