

Associations between clinical data, vaccination status, antibody responses, and post-COVID-19 symptoms in Thais infected with SARS-CoV-2 Delta and Omicron variants: a 1-year follow-up study
- PMID: 39375604
- PMCID: PMC11460119
- DOI: 10.1186/s12879-024-09999-2
Associations between clinical data, vaccination status, antibody responses, and post-COVID-19 symptoms in Thais infected with SARS-CoV-2 Delta and Omicron variants: a 1-year follow-up study
Abstract
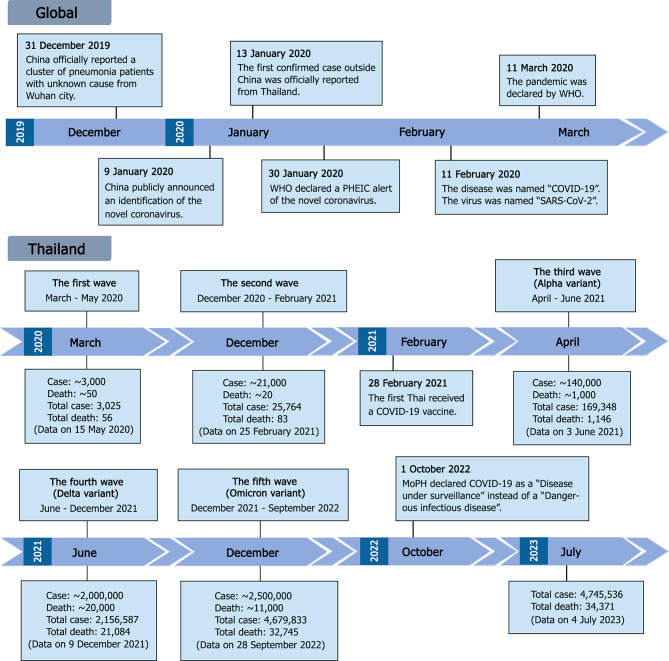
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19), led to a global pandemic from 2020. In Thailand, five waves of outbreaks were recorded, with the fourth and fifth waves driven by the Delta and Omicron variants, resulting in over 20,000 new confirmed cases daily at their peaks.
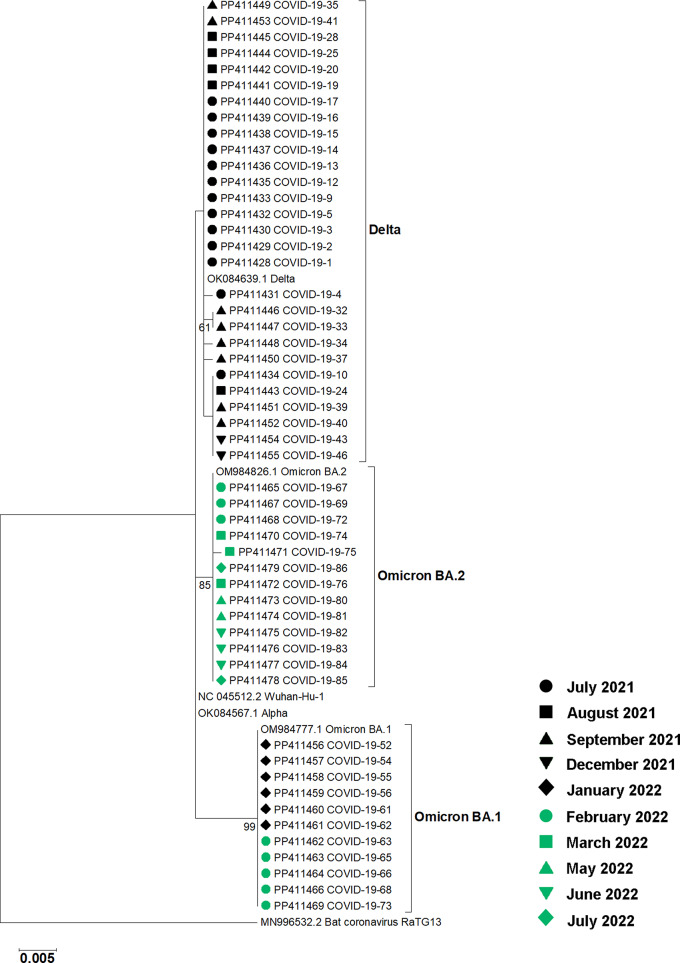
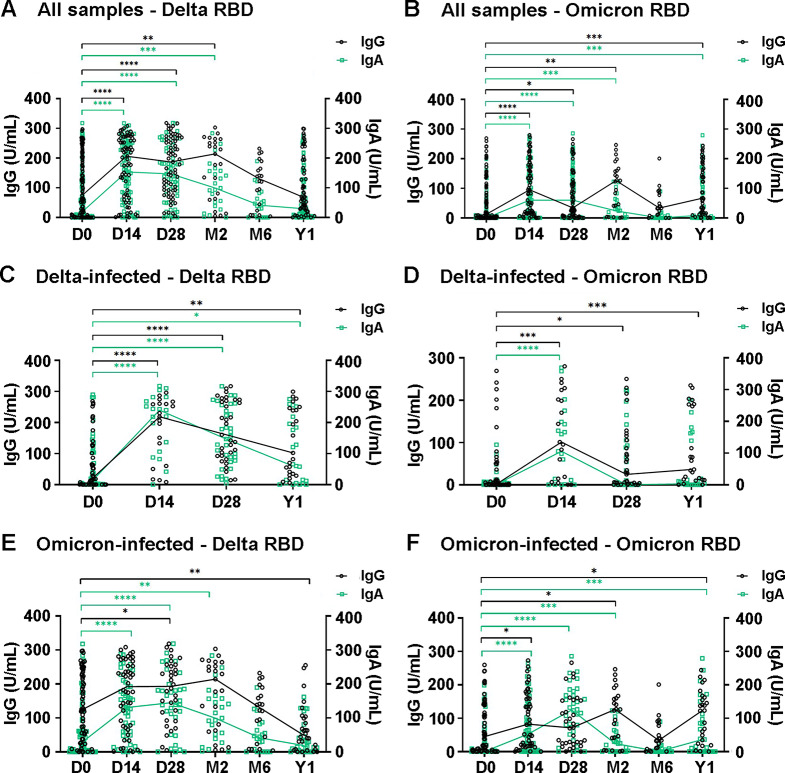
Methods: This cross-sectional study investigated the associations between clinical symptoms, vaccination status, antibody responses, and post-COVID-19 sequelae in COVID-19 patients. Plasma samples and clinical data were collected from participants admitted to hospitals in Thailand between July 2021 and August 2022, with follow-ups conducted for one year. The study included 110 participants infected with either the Delta (n = 46) or Omicron (n = 64) variants. Virus genotypes were confirmed by RT-PCR of nasal swab RNA and partial nucleotide sequencing of the S gene. IgG and IgA antibody levels against the receptor-binding domain (RBD) of SARS-CoV-2 Delta and Omicron variants were measured in plasma samples using ELISA.
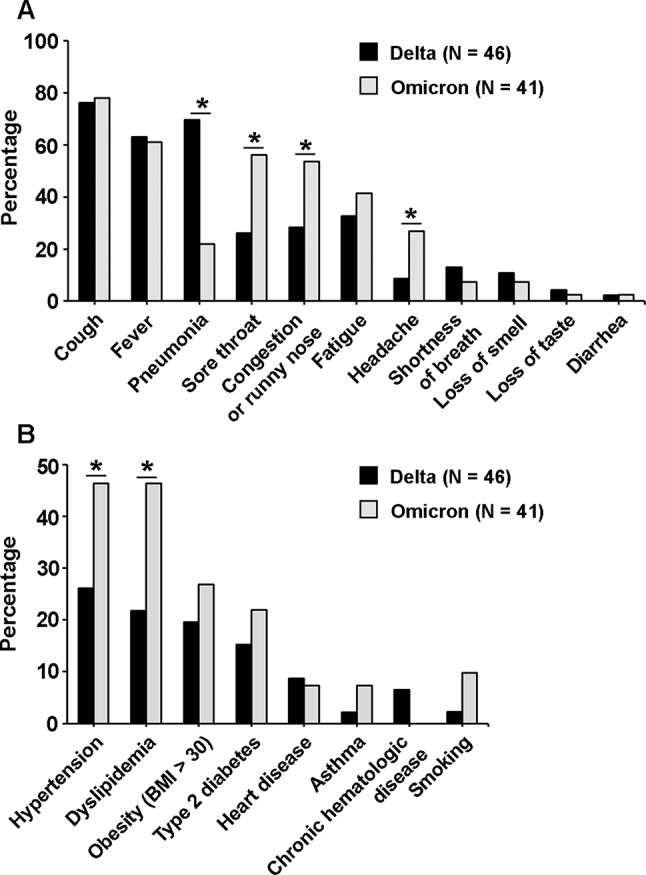
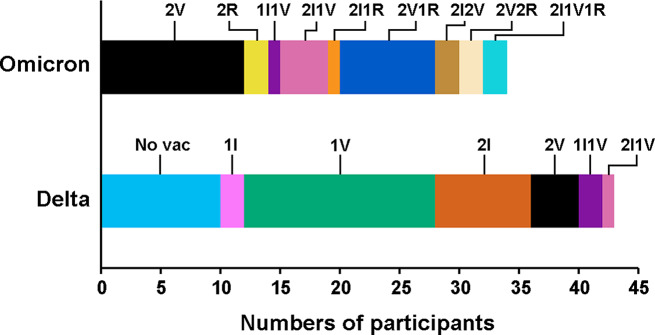
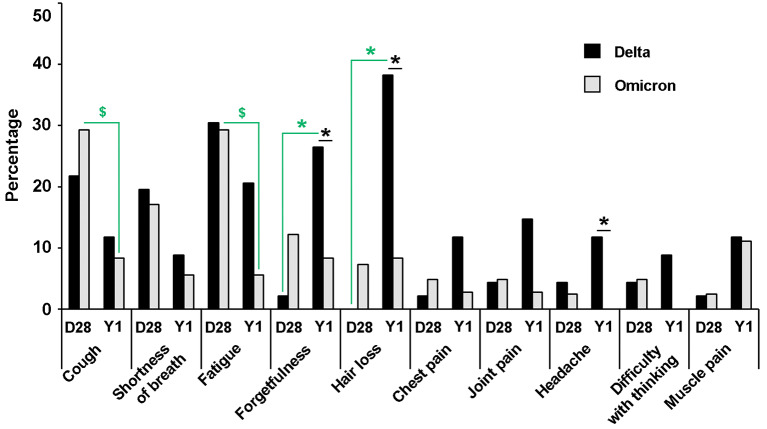
Results: Pneumonia was found to be associated with Delta variant infections, while sore throat, congestion or runny nose, and headache were linked to Omicron infections. Vaccination with fewer than two doses and diabetes mellitus were significantly associated with higher disease severity. Specific IgG and IgA antibodies against the RBD of the Delta variant generally rose by day 14 and were maintained for up to two months, whereas the pattern of antibody response to the Omicron variant was less clear. Antibody risings were found to be positively associated with pneumonia, certain underlying conditions (obesity, hypertension, dyslipidemia, and diabetes mellitus), and age ≥ 60 years. Delta variant infections were associated with forgetfulness, hair loss, and headache during the 1-year post-infection period. Females were more likely to experience hair loss, forgetfulness, and joint pain, while older age was associated with joint pain.
Conclusions: This study enhances our understanding of SARS-CoV-2 infections in Thais, particularly concerning the Delta and Omicron variants. The findings can inform public health planning and response strategies for future outbreaks of SARS-CoV-2 or other emerging viral diseases.
Keywords: Antibody response; COVID-19; Delta; ELISA; Omicron; SARS-CoV-2; Thailand.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ortiz-Prado E, Simbaña-Rivera K, Gómez-Barreno L, Rubio-Neira M, Guaman LP, Kyriakidis NC, et al. Clinical, molecular, and epidemiological characterization of the SARS-CoV-2 virus and the Coronavirus Disease 2019 (COVID-19), a comprehensive literature review. Diagn Microbiol Infect Dis. 2020;98:115094. - PMC - PubMed
-
- Mohan BS, Nambiar V. COVID-19: an insight into SARS-CoV-2 pandemic originated at Wuhan city in Hubei Province of China. J Infect Dis Epidemiol. 2020;6:146.
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
