

Residual diabetic foot osteomyelitis after surgery leads to poor clinical outcomes: A systematic review and meta-analysis
- PMID: 39376015
- PMCID: PMC11584361
- DOI: 10.1111/wrr.13215
Residual diabetic foot osteomyelitis after surgery leads to poor clinical outcomes: A systematic review and meta-analysis
Abstract
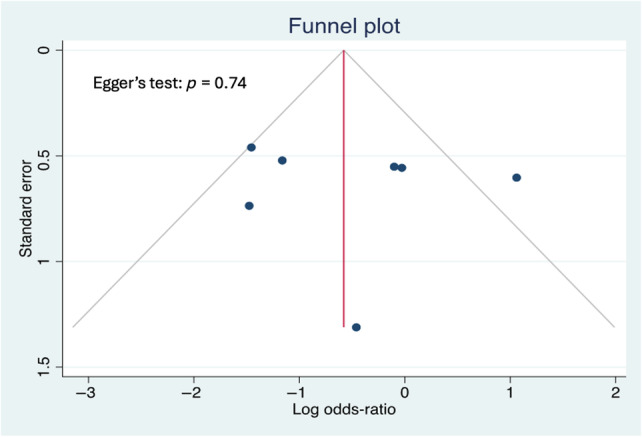
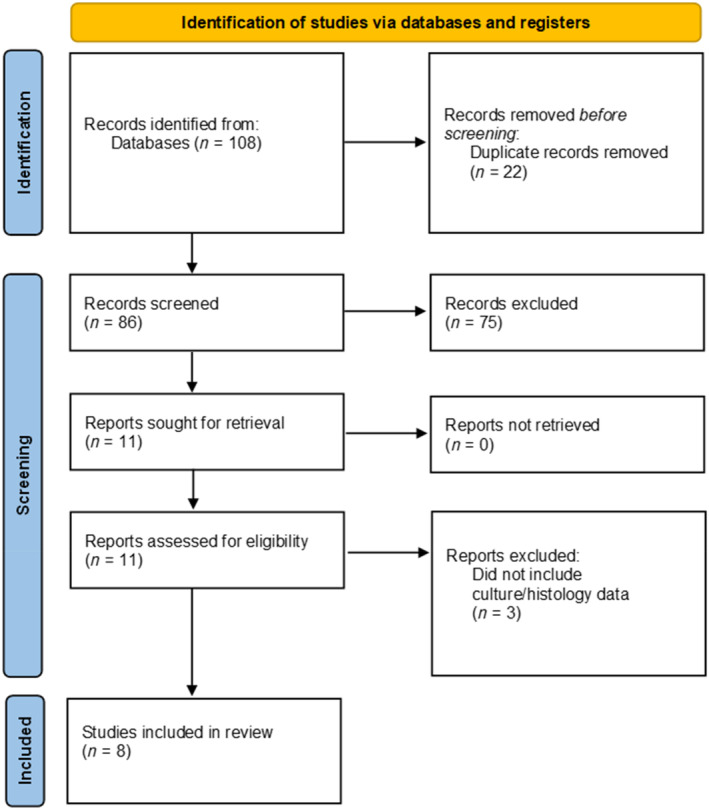
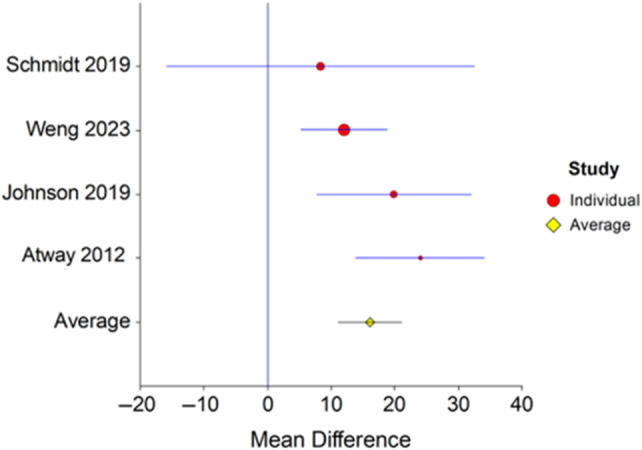
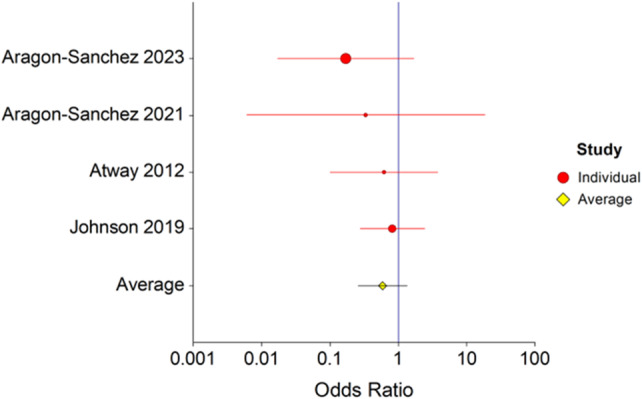
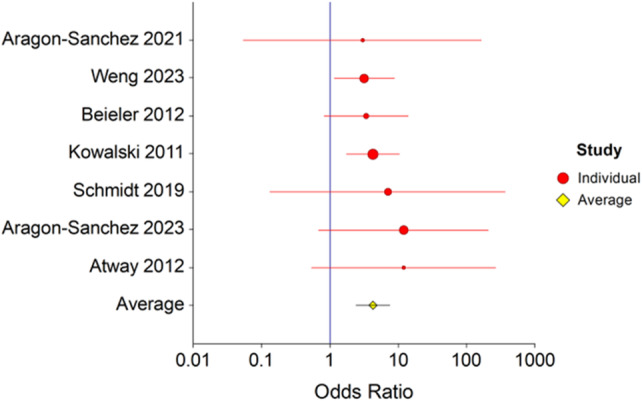
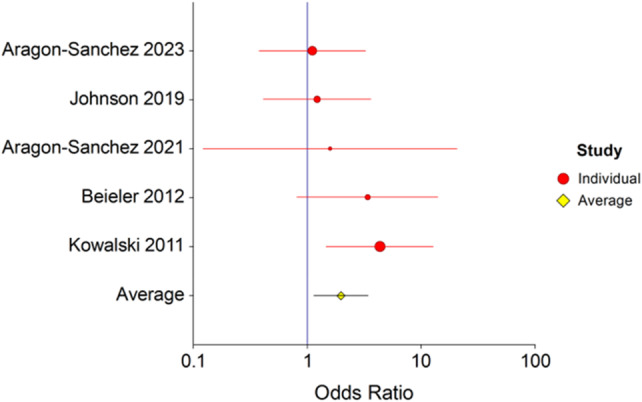
The aim of this meta-analysis is to compare the clinical outcomes in patients with and without residual osteomyelitis (ROM) after surgical bone resection for diabetic foot osteomyelitis (DFO). We completed a systematic literature search using PubMed, Scopus, and Embase using keywords DFO, Residual OM (ROM), and positive bone margins. The study outcomes included wound healing, antibiotic duration, amputation, and re-infection. Five hundred and thirty patients were included in the analysis; 319 had no residual osteomyelitis (NROM), and 211 had ROM. There was not a significant difference in the proportion of wounds that healed 0.6 (p = 0.1, 95% confidence intervals [95% CI] 0.3-1.3). The risk of infection was 2.0 times higher (OR = 2.0, p = 0.02, 95% CI 1.1-3.4), and the risk of amputation was 4.3 times higher (OR = 4.3, p = 0.0001, 95% CI 2.4-7.6) in patients with ROM. Patients with ROM received antibiotics significantly longer. The mean difference was 16.3 days (p = 0.02, 95% CI 11.1-21.1).
Keywords: amputation; diabetes; foot ulcer; infection; neuropathy; osteomyelitis.
© 2024 The Author(s). Wound Repair and Regeneration published by Wiley Periodicals LLC on behalf of The Wound Healing Society.
Conflict of interest statement
No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
