

Recognition of dural to pial supply in high-grade dural arteriovenous fistula: A technical note
- PMID: 39376095
- PMCID: PMC11559922
- DOI: 10.1177/15910199241272596
Recognition of dural to pial supply in high-grade dural arteriovenous fistula: A technical note
Abstract
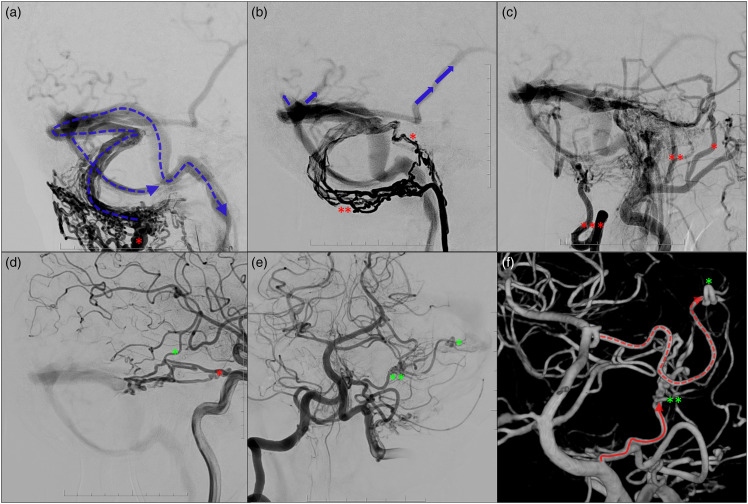
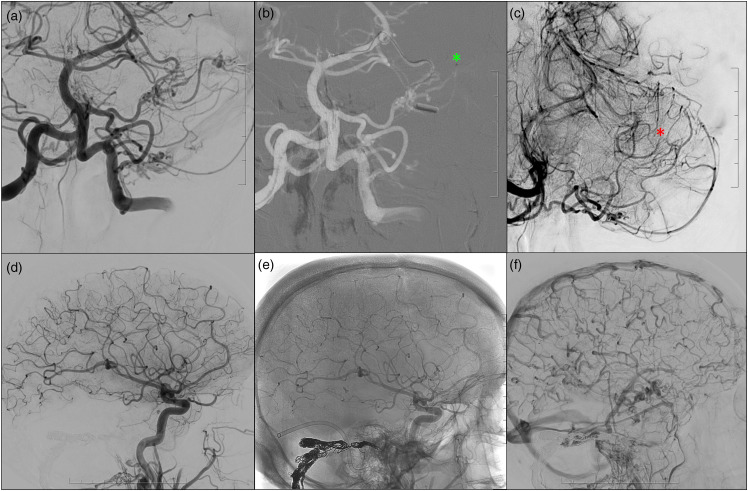
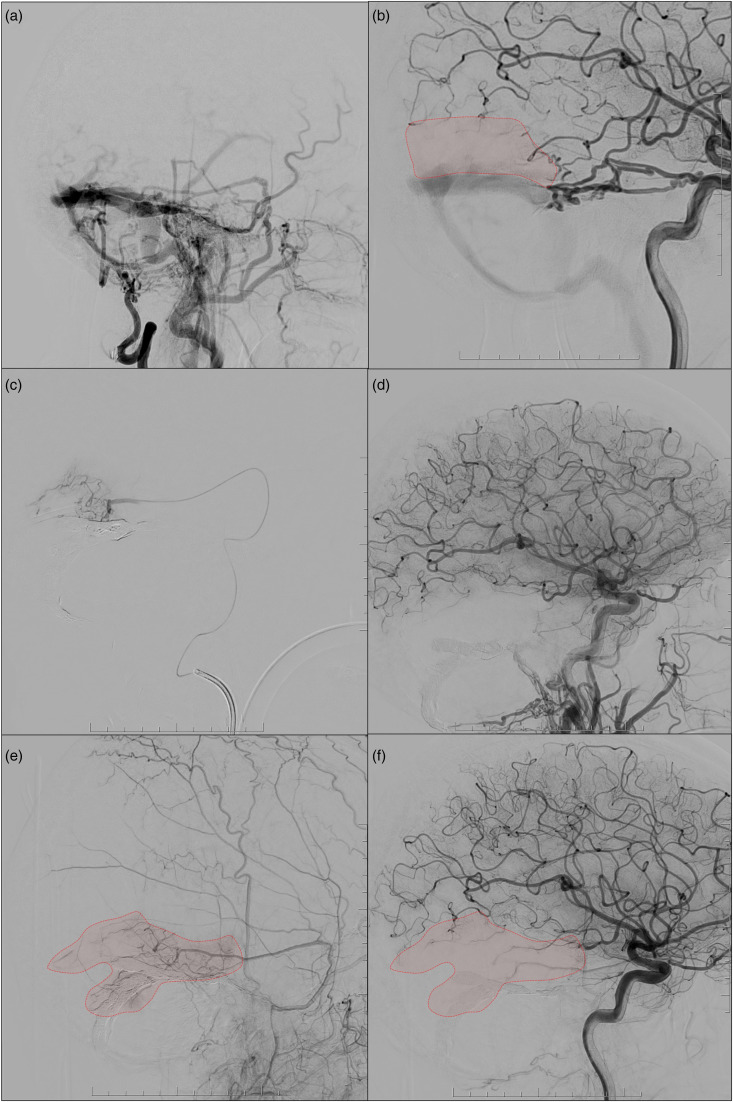
High-grade dural arteriovenous fistulas (DAVFs) are known to demonstrate classical dural supply and can demonstrate pre-existing dural supply and 'pure' arterial supply from pial branches. The latter two are examples of congenital versus acquired pial to dural shunting, respectively. We describe the recognition of dural to pial supply during combined transarterial and transvenous embolization of a high-grade DAVF with holocephalic venous reflux, stressing the importance of careful assessment of this condition with micro catheter injections.
Keywords: Dural arteriovenous fistula; VEGF; dural supply; endovascular treatment; pial supply.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EH is consultant for Medtronic.
Figures
References
-
- van Dijk JMC, terBrugge KG, Willinsky RA, et al. Clinical course of cranial dural arteriovenous fistulas with long-term persistent cortical venous reflux. Stroke 2002; 33: 1233–1236. - PubMed
-
- Osada T, Krings T. Intracranial dural arteriovenous fistulas with pial arterial supply. Neurosurgery 2019; 84: 104–115. - PubMed
-
- Brinjikji W, Cloft HJ, Lanzino G. Clinical, angiographic, and treatment characteristics of cranial dural arteriovenous fistulas with pial arterial supply. J Neurointerv Surg 2021; 13: 331–335. 20200629. - PubMed
-
- Wu Q, Zhang X-S, Wang H-D, et al. Onyx embolization for tentorial dural arteriovenous fistula with pial arterial supply: case series and analysis of complications. World Neurosurg 2016; 92: 58–64. 20160420. - PubMed
LinkOut - more resources
Full Text Sources
