

Improving Adherence and Reducing Health Care Costs Through Blister-Packaging: An Economic Model for a Commercially Insured Health Plan
- PMID: 39376478
- PMCID: PMC11457784
- DOI: 10.2147/CEOR.S480890
Improving Adherence and Reducing Health Care Costs Through Blister-Packaging: An Economic Model for a Commercially Insured Health Plan
Abstract
Purpose: To model the potential clinical and economic impact of blister-packaging medications for chronic conditions on medication adherence and healthcare costs in a commercially insured population.
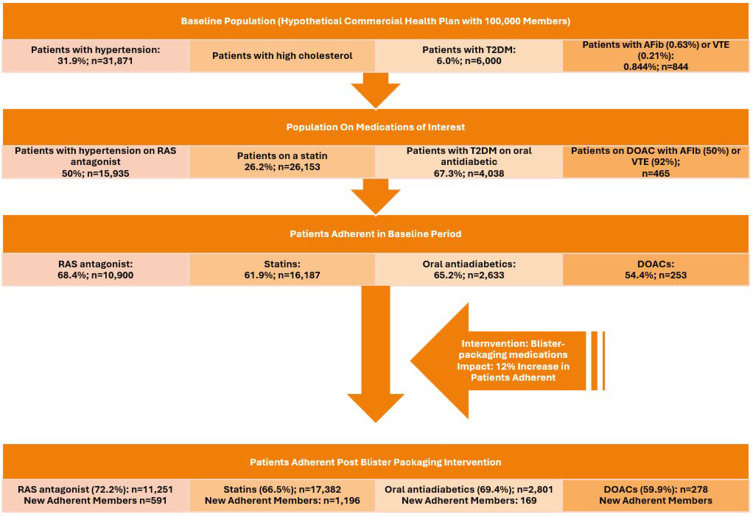
Methods: A health economic model was developed to evaluate the potential impact of blister-packaging chronic medications for a commercially insured population. The chronic medication classes assessed were renin-angiotensin-system (RAS) antagonists, statins, non-insulin oral antidiabetics, and direct oral anticoagulants (DOACs). The model was designed to reflect the perspective of a hypothetical commercially insured health plan with 100,000 members, over a one-year time horizon. Literature-based or best available epidemiologic references were used to inform the number of patients utilizing each medication class, the impact of blister-packaging on the number of patients who become adherent, as well as the impact of medication adherence in a commercially insured population on healthcare costs for each medication class assessed. Impact on costs was measured in total net healthcare costs, as well as being stratified by medical costs and medication costs.
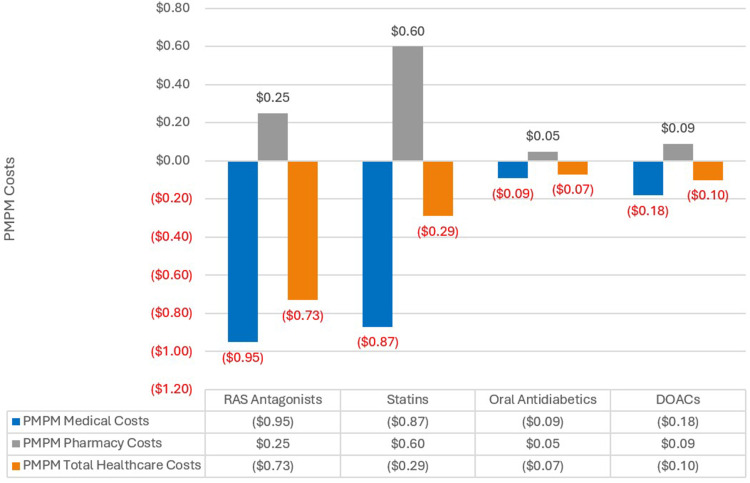
Results: Following the blister-packaging intervention, there were an additional 591 patients adherent to RAS antagonists, 1196 patients adherent to statins, 169 patients adherent to oral antidiabetics, and 25 patients adherent to DOACs. While pharmacy costs increased, these costs were more than offset by the reduction in medical costs. Overall, the increase in patients adherent to therapy due to blister-packaging led to a reduction in total healthcare costs of $879,312 for RAS antagonists (-$0.73 per-member per-month (PMPM)), $343,322 for statins (-$0.29 PMPM), $78,917 for oral antidiabetics (-$0.07 PMPM), and $120,793 for DOACs (-$0.10 PMPM).
Conclusion: Blister-packaging chronic medications in a commercially insured population has the potential to reduce healthcare costs. Future research is needed to confirm these findings in real-world settings and to fully understand the clinical and economic implications of blister-packaging chronic medications.
Keywords: blister-packaging; blister-packing; healthcare costs; medical cost offsets; medication adherence; medication adherence packaging; self-insured; total cost of care.
Plain language summary
Patients not taking their medications as prescribed is common in the United States, leading to disease progression, increased healthcare visits, and increased healthcare costs. Blister-packaging medications is an intervention shown to increase medication adherence, or patients taking their medication as prescribed, and has been around for several decades. While there is research and literature available that shows the impact that blister-packaging medications has on improving adherence, and there is literature available that shows patients taking their medications as prescribed reduces healthcare costs, there is minimal literature available that directly ties these two concepts together. As a result, we modeled from a hypothetical commercial insurance health plan perspective what the impact would be of blister-packaging chronic medications on healthcare costs using the best available peer-reviewed literature and epidemiologic data. This analysis found that for a commercially insured health plan with 100,000 members, 591 additional patients would become adherent to their renin-angiotensin-system (RAS) antagonists blood pressure medications, 1196 additional patients would become adherent to their statins, 169 additional patients would become adherent to their oral antidiabetics, and 25 additional patients would become adherent to their direct oral anticoagulants (DOACs). Additionally, this would lead to a reduction in healthcare costs for the health plan of $879,312 for RAS antagonists (-$0.73 per-member per-month (PMPM)), $343,322 for statins (-$0.29 PMPM), $78,917 for oral antidiabetics (-$0.07 PMPM), and $120,793 for DOACs (-$0.10 PMPM).
© 2024 Borrelli et al.
Conflict of interest statement
Saad, Dumitru, and Lucaci are employees and shareholders of Becton, Dickinson and Company. Borrelli and Barnes are employees of Becton, Dickinson and Company. Barnes is a shareholder of BioMérieux. No other conflicts of interest to report.
Figures
Similar articles
-
Estimating the economic impact of blister-packaging on medication adherence and health care costs for a Medicare Advantage health plan.J Manag Care Spec Pharm. 2024 Dec;30(12):1442-1454. doi: 10.18553/jmcp.2024.24179. Epub 2024 Sep 11. J Manag Care Spec Pharm. 2024. PMID: 39258999 Free PMC article.
-
Enhancing Outcomes in Opioid Use Disorder Treatment: An Economic Evaluation of Improving Medication Adherence for Buprenorphine Through Blister-Packaging.Subst Abuse Rehabil. 2024 Oct 22;15:209-222. doi: 10.2147/SAR.S484831. eCollection 2024. Subst Abuse Rehabil. 2024. PMID: 39463862 Free PMC article.
-
Enhancing medication adherence with blister-packed oral oncolytics: A case example in chronic lymphocytic leukemia.J Oncol Pharm Pract. 2025 Feb 19:10781552241306704. doi: 10.1177/10781552241306704. Online ahead of print. J Oncol Pharm Pract. 2025. PMID: 39969400
-
Evaluating the efficacy of blister packaging in improving medication adherence within psychiatry: A systematic literature review.Ment Health Clin. 2025 Jun 2;15(3):176-186. doi: 10.9740/mhc.2025.06.176. eCollection 2025 Jun. Ment Health Clin. 2025. PMID: 40496006 Free PMC article. Review.
-
Systematic Review of Real-World Treatment Patterns of Oral Antipsychotics and Associated Economic Burden in Patients with Schizophrenia in the United States.Adv Ther. 2022 Sep;39(9):3933-3956. doi: 10.1007/s12325-022-02232-z. Epub 2022 Jul 18. Adv Ther. 2022. PMID: 35844007 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
