

Risk for Suicide Attempts Assessed Using the Patient Health Questionnaire-9 Modified for Teens
- PMID: 39378032
- PMCID: PMC11581555
- DOI: 10.1001/jamanetworkopen.2024.38144
Risk for Suicide Attempts Assessed Using the Patient Health Questionnaire-9 Modified for Teens
Abstract
Importance: Suicide is a leading cause of death in US youths.
Objective: To assess whether screening with supplemental items 10 to 13 on the Patient Health Questionnaire-9 modified for teens (PHQ-9M) improves prediction of youth suicide attempts beyond the information provided by the first 9 items alone (the PHQ-9).
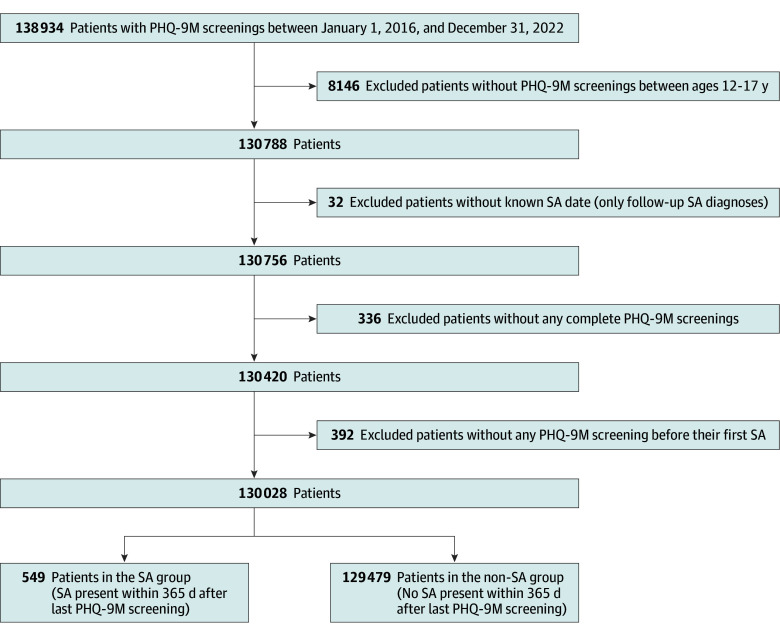
Design, setting, and participants: This retrospective cohort study used a retrospective cohort of adolescents aged 12 to 17 years who were screened for depression in outpatient facilities within a pediatric health care system between January 1, 2016, and December 31, 2022, with up to 1 year of follow-up to assess the occurrence of suicidal behavior. Follow-up was completed on December 31, 2023.
Exposure: Screening with the PHQ-9M.
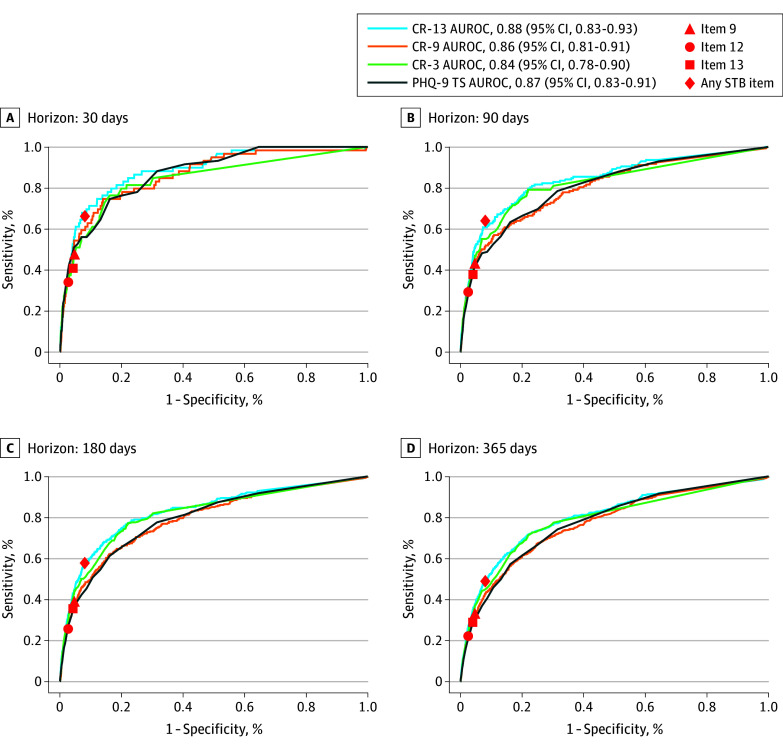
Main outcomes and measures: This study developed and compared prediction using 3 Cox proportional hazards regression models (CR-9, CR-13, and CR-3) of subsequent suicide attempts, determined by the hospital's electronic health records up to 1 year following the last PHQ-9M screening. The CR-9 model used the PHQ-9 and the CR-13 model used all 13 items of PHQ-9M. The CR-3 model used the 3 most impactful variables selected from the 13 PHQ-9M items and PHQ-9 total score. All models were evaluated across 4 prediction horizons (30, 90, 180, and 365 days) following PHQ-9M screenings. Evaluation metrics were the area under the receiver operating characteristic curve (AUROC) and the area under the precision recall curve (AUPRC).
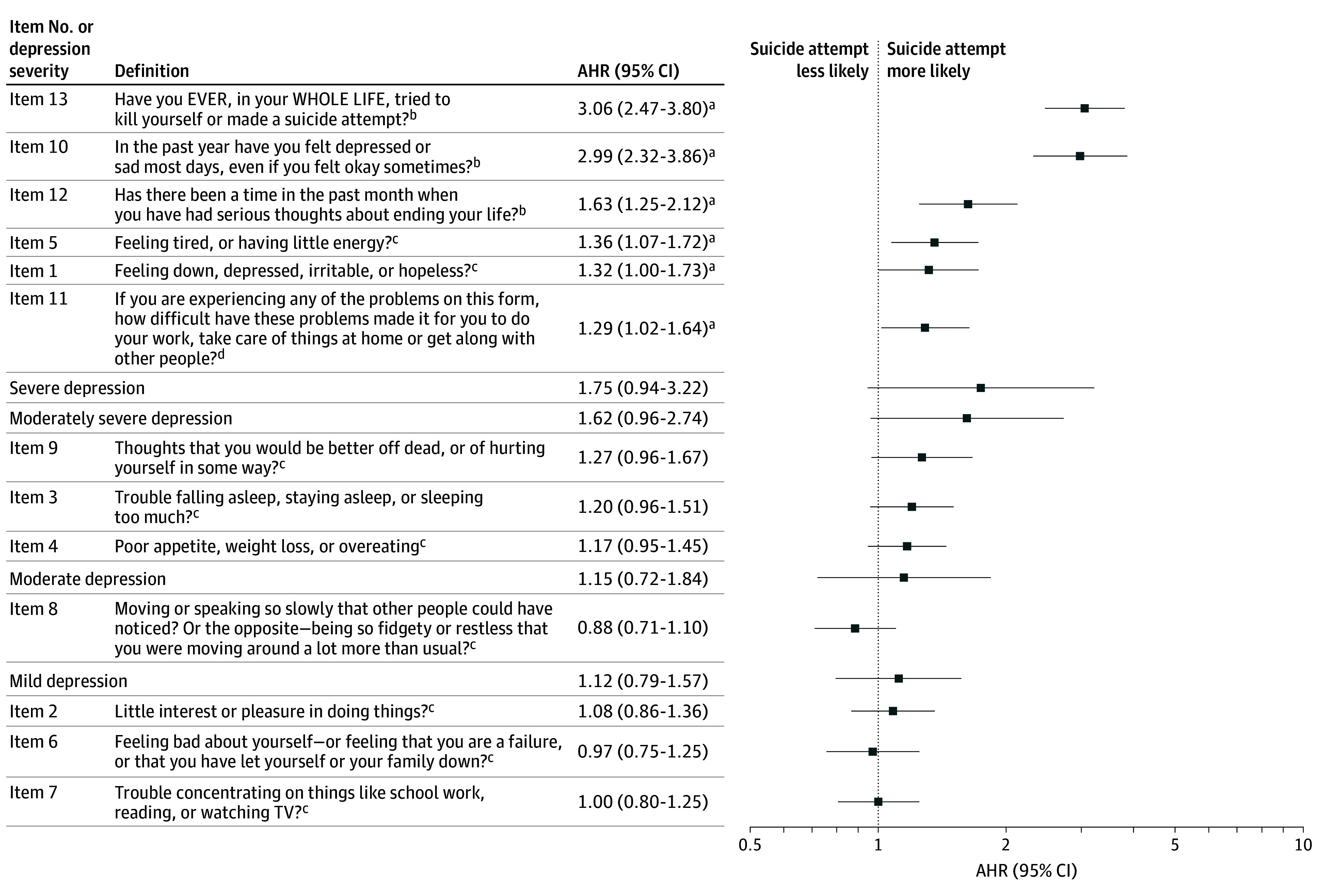
Results: Of 130 028 outpatients (65 520 [50.4%] male) with 272 402 PHQ-9M screenings, 549 (0.4%) had subsequent suicide attempts within 1 year following the PHQ-9M screening. The AUROC of the CR-9 model in the 365-day horizon was 0.77 (95% CI, 0.75-0.79); of the CR-13 model, 0.80 (95% CI, 0.78-0.82); and of the CR-3 model, 0.79 (95% CI, 0.76-0.81); the AUPRC of the CR-9 model was 0.02 (95% CI, 0.02-0.03); of the CR-13 model, 0.03 (95% CI, 0.02-0.03); and of the CR-3 model, 0.02 (95% CI, 0.02-0.03). The 3 most impactful items using adjusted hazard ratios were supplemental item 13 (lifetime suicide attempts; 3.06 [95% CI, 2.47-3.80]), supplemental item 10 (depressed mood severity in the past year; 2.99 [95% CI, 2.32-3.86]), and supplemental item 12 (serious suicidal ideation in the past month; 1.63 [95% CI, 1.25-2.12]). All of the models achieved higher AUROCs as prediction horizons shortened.
Conclusions and relevance: In this cohort study of adolescent PHQ-9M screenings, the supplemental items on PHQ-9M screening improved prediction of youth suicide attempts compared with screening using the PHQ-9 across all prediction horizons, suggesting that PHQ-9M screening should be considered during outpatient visits to improve prediction of suicide attempts.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention . Wide-ranging Online Data for Epidemiologic Research (WONDER): suicide rates between ages 12-17, 1999-2020. Accessed August 27, 2024. https://wonder.cdc.gov/ucd-icd10.html
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
