

Treatment strategy for cervical lymph node metastases from early-stage tongue and floor of the mouth squamous cell carcinoma using tumour budding and depth of invasion as predictors
- PMID: 39379623
- PMCID: PMC11461577
- DOI: 10.1007/s00784-024-05974-y
Treatment strategy for cervical lymph node metastases from early-stage tongue and floor of the mouth squamous cell carcinoma using tumour budding and depth of invasion as predictors
Abstract
Objectives: This study aimed to determine whether elective neck dissection can help improve outcomes in early-stage tongue and floor squamous cell carcinoma (SCC) by statistically analysing the relationship between information obtained from biopsy specimens and the incidence and prognosis of cervical lymph node metastasis (CLM).
Materials and methods: Biopsy specimens of 103 patients diagnosed with early cT1-T2 cancer of the tongue and floor of the mouth were included.
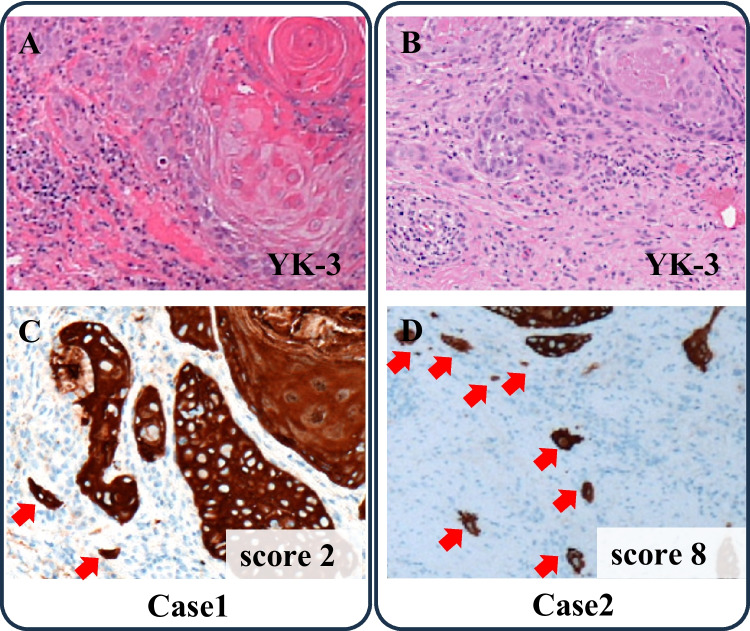
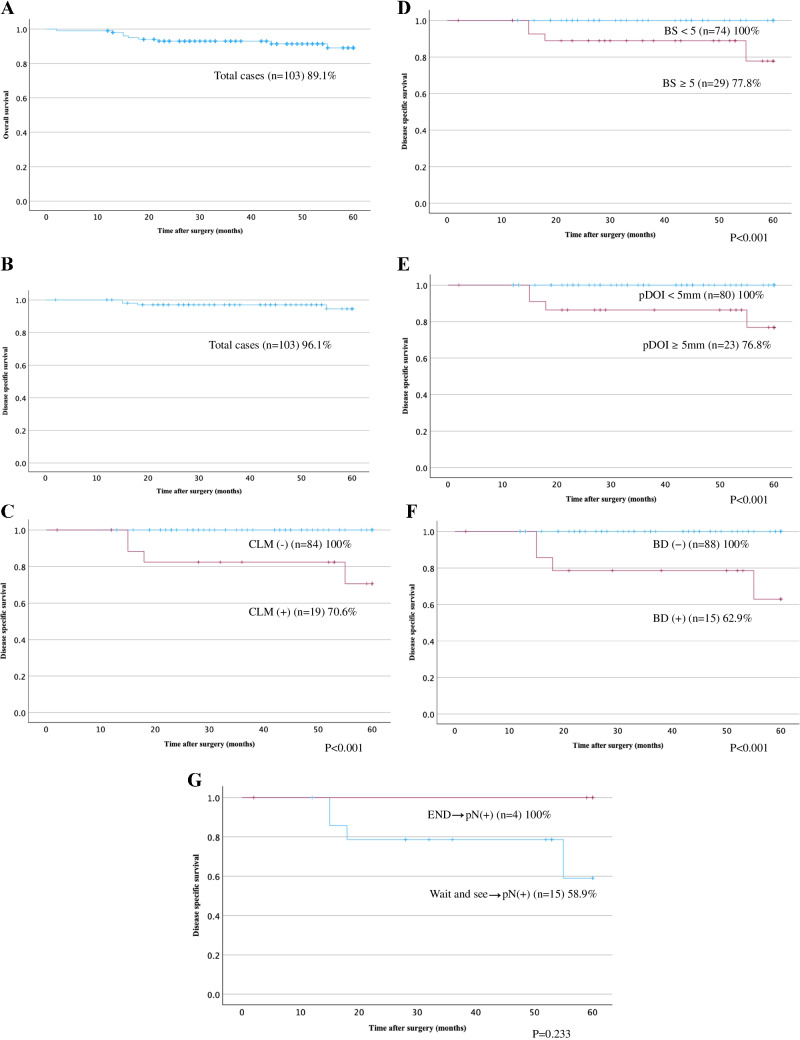
Results: Multivariate analysis showed that the three parameters significantly correlated with CLM, and univariate analyses showed that budding score (BS) ≥ 5 and pathological depth of invasion (pDOI) ≥ 5 mm were independent risk factors for CLM. There were significant differences in the 5-year cumulative disease-specific survival between the BS < 5 and BS ≥ 5 groups, the pDOI < 5 mm and pDOI ≥ 5 mm groups, and the positive and negative budding and depth of invasion (BD) score groups.
Conclusion: In early-stage tongue and floor of the mouth cancers with maximum tumour diameter ≤ 20 mm, it may be necessary to treat occult CLM during initial surgery based on the following preoperative criteria: pDOI ≥ 5 mm or BS ≥ 5 in biopsy specimens and DOI ≥ 8 mm on imaging. The BD model exhibited the highest specificity and proved helpful for CLM prediction.
Clinical relevance: pDOI ≥ 5 mm and BS ≥ 5 were independent predictors of CLM and prognosis in early-stage tongue and floor of the mouth cancers with a maximum tumour diameter of 20 mm.
Keywords: Biopsy; Cervical lymph node metastasis; Depth of invasion; Early tongue and floor of the mouth squamous cell carcinoma; Tumour budding.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Tanaka K, Hanai N, Eba J, Mizusawa J, Asakage T, Homma A, Kiyota N, Fukuda H, Hayashi R (2018) Randomized phase III study to evaluate the value of omission of prophylactic neck dissection for stage I/II tongue cancer: Japan Clinical Oncology Group study (JCOG1601, RESPOND). Jpn J Clin Oncol 48:1105–1108. 10.1093/jjco/hyy125 - DOI - PubMed
-
- Ganly I, Goldstein D, Carlson DL, Patel SG, O’Sullivan B, Lee N, Gullane P, Shah JP (2013) Long-term regional control and survival in patients with “low-risk,” early stage oral tongue cancer managed by partial glossectomy and neck dissection without postoperative radiation: the importance of tumor thickness. Cancer 119:1168–1176. 10.1002/cncr.27872 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
