

Surgical interventions for degenerative lumbar spinal stenosis: a systematic review with network meta-analysis
- PMID: 39379938
- PMCID: PMC11463109
- DOI: 10.1186/s12916-024-03653-z
Surgical interventions for degenerative lumbar spinal stenosis: a systematic review with network meta-analysis
Abstract
Background: Several surgical options for degenerative lumbar spinal stenosis (LSS) are available, but current guidelines do not recommend which one should be prioritized. Although previous network meta-analyses (NMAs) have been performed on this topic, they have major methodological problems and could not provide the convincing evidence and clinical practical information required.
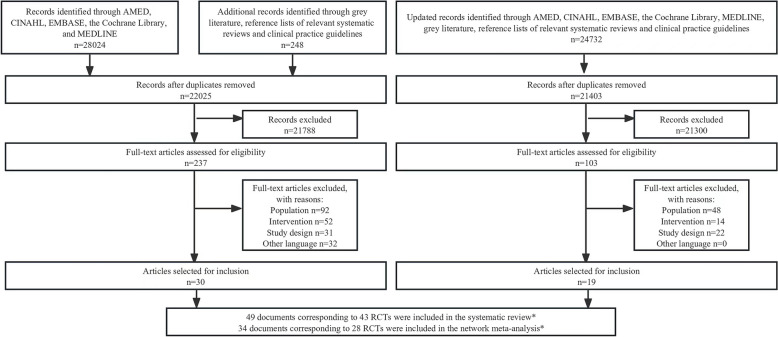
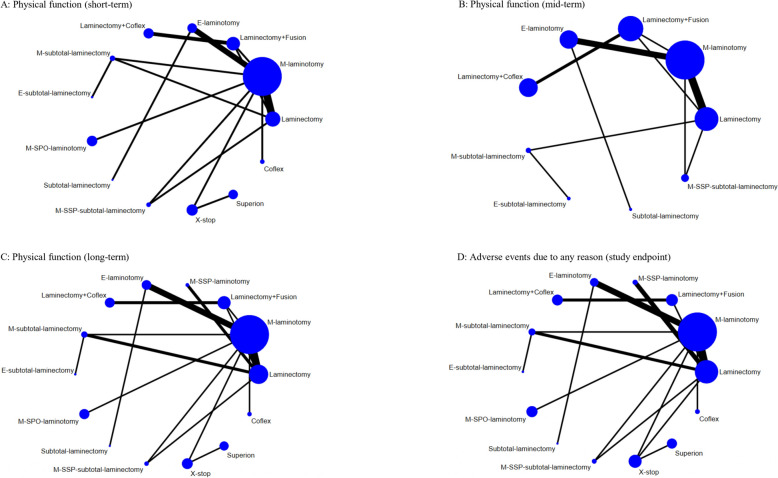
Methods: Randomized controlled trials (RCTs) comparing at least two surgical interventions were included by searching AMED, CINAHL, EMBASE, the Cochrane Library, and MEDLINE (inception to August 2023). A frequentist random-effects NMA was performed for physical function and adverse events due to any reason. For physical function, three follow-up time points were included: short-term (< 6 months post-intervention), mid-term (≥ 6 months but < 12 months), and long-term (≥ 12 months). Laminectomy was the reference comparison intervention.
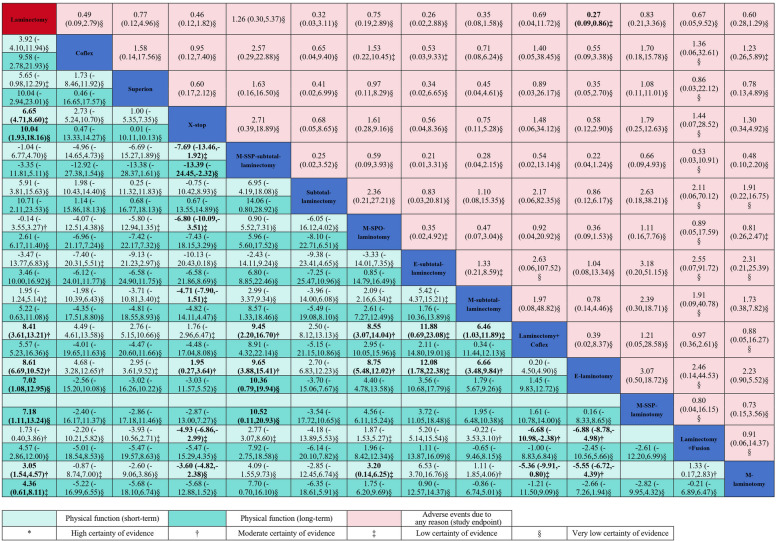
Results: A total of 43 RCTs involving 5017 participants were included in the systematic review and 28 RCTs encompassing 14 types of surgical interventions were included in the NMA. For improving physical function (scale 0-100), endoscopic-assisted laminotomy (mean difference: - 8.61, 95% confidence interval: - 10.52 to - 6.69; moderate-quality evidence), laminectomy combined with Coflex (- 8.41, - 13.21 to - 3.61; moderate quality evidence), and X-stop (- 6.65, - 8.60 to - 4.71; low-quality evidence) had small effects at short-term follow-up; no statistical difference was observed at mid-term follow-up (very low- to low-quality evidence); at long-term follow-up, endoscopic-assisted laminotomy (- 7.02, - 12.95 to - 1.08; very low-quality evidence) and X-stop (- 10.04, - 18.16 to - 1.93; very low-quality evidence) had a small and moderate effect, respectively. Compared with laminectomy, endoscopic-assisted laminotomy was associated with fewer adverse events due to any reason (odds ratio: 0.27, 0.09 to 0.86; low-quality evidence).
Conclusions: For adults with degenerative LSS, endoscopic-assisted laminotomy may be the safest and most effective intervention in improving physical function. However, the available data were insufficient to indicate whether the effect was sustainable after 6 months.
Trial registration: PROSPERO (CRD42018094180).
Keywords: Lumbar spinal stenosis; Musculoskeletal disease; Network meta-analysis; Orthopaedics; Surgery; Systematic review.
© 2024. The Author(s).
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
