

Inflammation in liver fibrosis and atrial fibrillation: A prospective population-based proteomic study
- PMID: 39380717
- PMCID: PMC11460462
- DOI: 10.1016/j.jhepr.2024.101171
Inflammation in liver fibrosis and atrial fibrillation: A prospective population-based proteomic study
Abstract
Background & aims: Elevated liver stiffness has been associated with atrial fibrillation (AFib) in the general population. The mechanism underlying this association is unclear.
Methods: Participants were recruited from the general population and prospectively enrolled with follow-up for 5 years. The fibrosis-4 (FIB-4) index was used as a surrogate marker for liver fibrosis. Proteomics analysis was performed using the 92-target Olink inflammation panel. Validation was performed using the NAFLD fibrosis score (NFS), aspartate aminotransferase to platelet index (APRI), and repeat confirmation proteomics.
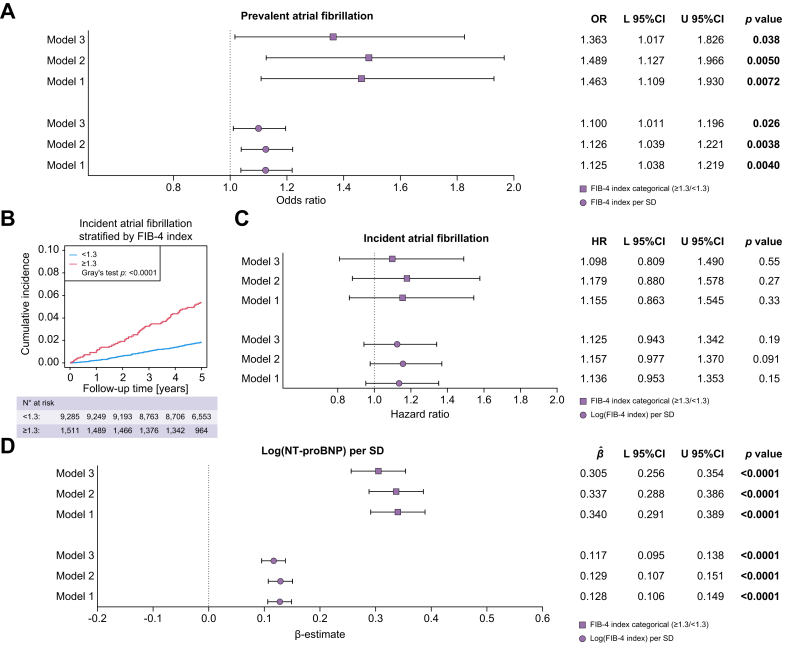
Results: A sample of 11,509 participants with a mean age of 54.0 ± 11.1 years, 51.3% women, and a median FIB-4 index of 0.85 (0.65/1.12), was used. The FIB-4 index was predictive for prevalent (FIB-4 index adjusted odds ratio (aOR) per SD: 1.100 with 95% CI 1.011-1.196; p = 0.026), but not incident AFib (log[FIB-4 index]) adjusted hazard ratio: 1.125 with 95% CI 0.943-1.342, p = 0.19). Elastic net regularized regression identified CCL20, DNER, and CXCL10 for prevalent AFib, and AXIN1, CXCL10, and Flt3L for the log(FIB-4 index) (per SD) as most important in common regulated proteins. The relationship between the FIB-4 index, the identified proteins, and AFib was relevant and reproduced at the 5-year follow-up for CXCL10 after adjusting for confounders (log[FIB-4 index] per SD - CXCL10 [per SD] adjusted β 0.160 with 95% CI 0.127-0.194, p <0.0001; CXCL10 [per SD] - AFib aOR 1.455 with 95% CI 1.217-1.741, p <0.0001), reproduced using the NFS and APRI, and corresponding to increased serum levels.
Conclusions: CXCL10 is linked to liver fibrosis, as determined by the FIB-4 index, and to prevalent AFib.
Impact and implications: How elevated liver stiffness relates to atrial fibrillation in the general population remains to be clarified. We hypothesized that systemic inflammation against a background of liver fibrosis produced from metabolic dysfunction-associated steatotic liver disease (MASLD), is involved in the pathophysiology of atrial fibrillation. Using large-scale targeted proteomics, we found that CXCL10 is related to both liver fibrosis, as defined by the fibrosis-4 index, and to atrial fibrillation. These results can aid evidence-based drug development for patients with atrial fibrillation and MASLD-related liver fibrosis.
Keywords: Atrial fibrillation; C-X-C motif chemokine ligand 10 (CXCL10); Fibrosis-4 index (FIB-4 index); Metabolic dysfunction-associated steatotic liver disease (MASLD); Non-invasive test; Proteomics.
© 2024 The Author(s).
Figures





References
-
- Anstee Q.M., Mantovani A., Tilg H., et al. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2018;15:425–439. - PubMed
-
- Boeckmans J., Sandrin L., Knackstedt C., et al. Liver stiffness as a cornerstone in heart disease risk assessment. Liver Int. 2024;44:344–356. - PubMed
-
- Brundel B.J.J.M., Ai X., Hills M.T., et al. Atrial fibrillation. Nat Rev Dis Primers. 2022;8:21. - PubMed
-
- Elliott A.D., Middeldorp M.E., Van Gelder I.C., et al. Epidemiology and modifiable risk factors for atrial fibrillation. Nat Rev Cardiol. 2023;6:404–417. - PubMed
-
- Wai-Sun Wong V., Ekstedt M., Lai-Hung Wong G., et al. Changing epidemiology, global trends and implications for outcomes of NAFLD. J Hepatol. 2023;79:842–852. - PubMed
LinkOut - more resources
Full Text Sources
