

Cerebrovascular pulsatility indicates preoperative subcortical cognitive impairment and an increased risk for postoperative delirium in elderly patients undergoing elective spine surgery
- PMID: 39380730
- PMCID: PMC11458395
- DOI: 10.3389/fmed.2024.1433380
Cerebrovascular pulsatility indicates preoperative subcortical cognitive impairment and an increased risk for postoperative delirium in elderly patients undergoing elective spine surgery
Abstract
Introduction: Advances in spine surgery enable safe interventions in elderly patients, but perioperative neurocognitive disorders (pNCD), such as post-operative delirium (POD) and cognitive dysfunction (POCD), remain a serious concern. Pre-operative cognitive impairment is a major risk factor for pNCD. Comprehensive pre-operative cognitive assessments are not feasible in clinical practice, making effective screening methods desirable. This study investigates whether pre-operative cerebrovascular duplex sonography can assess subcortical (vascular) cognitive impairment and the risk for POD.
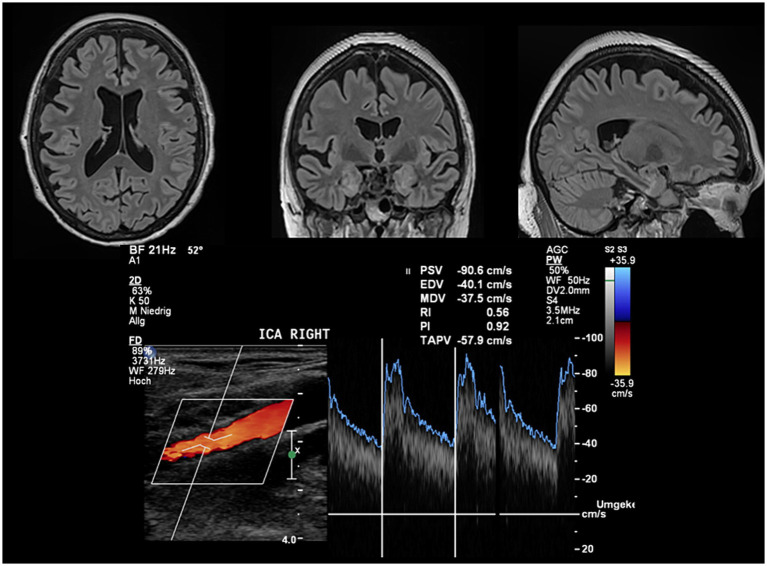
Methods: This prospective single-center study recruited patients aged ≥60 years scheduled for elective spine surgery at a German university hospital. Patients underwent pre-operative assessments including cognitive abilities (CERAD test battery), structural MRI, and cerebrovascular duplex sonography. POD screening was conducted three times daily for at least 3 days. The primary hypothesis, that the mean pulsatility index (PI) of both internal carotid arteries (ICA) predicts POD risk, was tested using logistic regression. Secondary analyses examined the association between POD risk and ICA flow (time-averaged peak velocities, TAPV) and correlations with cognitive profiles and MRI characteristics.
Results: POD occurred in 22% of patients (n = 22/99) within three postoperative days. Patients with POD were significantly older (75.9 ± 5.4 vs. 70.0 ± 6.9 years, p < 0.01) but did not differ by gender (p = 0.51). ICA PI significantly predicted POD risk (OR = 5.46 [95%CI: 1.81-16.49], p = 0.003), which remained significant after adjustment for age and duration of surgery (ORadj = 6.38 [95% CI: 1.77-23.03], p = 0.005). TAPV did not inform the POD risk (p = 0.68). ICA PI Pre-operative cognitive scores were significantly associated with ICA PI (mean CERAD score: r = -0.32, p < 0.001). ICA PI was also significantly associated with total white matter lesion volume (τ = 0.19, p = 0.012) and periventricular white matter lesion volume (τ = 0.21, p = 0.007).
Discussion: This is the first study to demonstrate that cerebrovascular duplex sonography can assess the risk for POD in elderly spine surgery patients. Increased ICA PI may indicate subcortical impairment, larger white matter lesion load, and lower white matter volume, predisposing factors for POD. Pre-operative cerebrovascular duplex sonography of the ICA is widely available, easy-to-use, and efficient, offering a promising screening method for POD risk. Increased ICA PI could supplement established predictors like age to adjust surgical and peri-operative procedures to individual risk profiles.
Keywords: carotid ultrasound; cognitive impairment; delirium; risk prediction; spine surgery; white matter lesions.
Copyright © 2024 Saar, Müller, Veser, Behr, Rathmann, Schroeder, Flöel, Müller, von Sarnowski and Fleischmann.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Muller J, Nowak S, Weidemeier M, Vogelgesang A, Ruhnau J, von Sarnowski B, et al. , Duration of Surgery and Intraoperative Blood Pressure Management are Modifiable Risk Factors for Postoperative Neurocognitive Disorders Following Spine Surgery: Results of the Prospective CONFESS Study. Spine (Phila Pa 1976). (2023) - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous