

Ballistic Nerve Injuries: State of the Evidence and Approach to the Patient Based on Experience
- PMID: 39381398
- PMCID: PMC11456629
- DOI: 10.1016/j.jhsg.2024.01.021
Ballistic Nerve Injuries: State of the Evidence and Approach to the Patient Based on Experience
Abstract
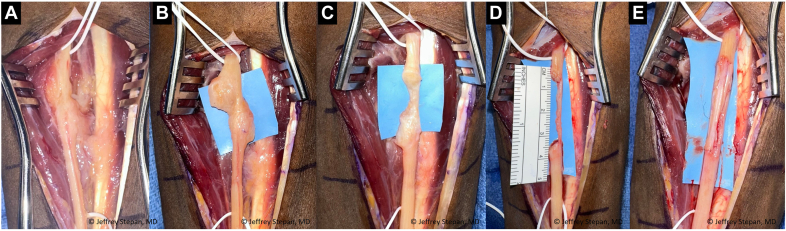
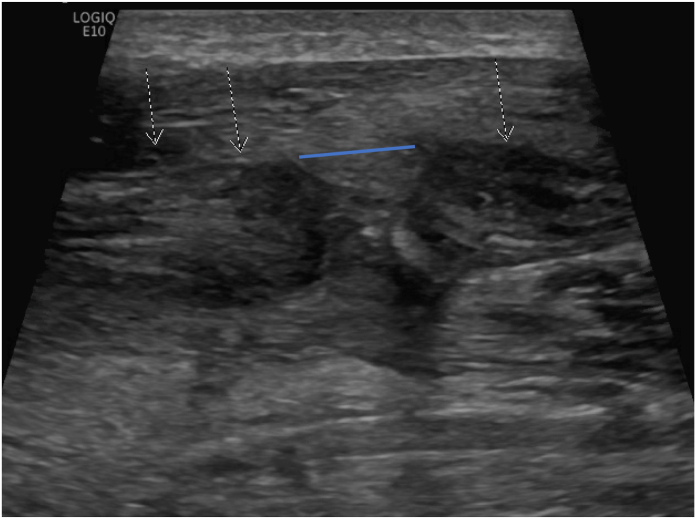
Nerve injuries secondary to gunshot wounds (GSWs) have been traditionally thought of as neurapraxic injuries with high likelihood of complete recovery. A review of the literature, however, highlights the misconceptions surrounding ballistic nerve injuries and their treatments. Contrary to this accepted dogma, approximately 30% to 60% of GSWs to the upper extremity may result in nerve injury requiring repair or reconstruction. Surgical exploration following ballistic injury reveals that 20% to 55% of nerves were lacerated requiring repair or grafting. Despite these numbers, outcomes after nerve repair or grafting are limited, and the limited data show evidence of poor functional recovery. In our experience, delayed exploration of GSW-related nerve injuries in patients without signs of functional recovery demonstrate large neuromas in continuity often requiring meticulous dissection and excision with resulting large gaps that require reconstruction. This has led us to explore options to identify patients with nerve deficits after GSWs who may benefit from earlier exploration. Others advocate for the exploration of all ballistic nerve injuries, which would represent a logistical challenge in high volume centers and may lead to unnecessary explorations of in continuity nerves. To facilitate identification of nerve injury following GSWs, we have explored the utilization of early ultrasound to identify patients with nerve lacerations that may benefit from early exploration (1-2 weeks after injury). Earlier exploration can lead to less technically challenging surgery, shorter nerve gaps, and more time for the nerve to recover. Herein, we present a series of cases to help illustrate this approach to the patient. Although early exploration and repair versus grafting of nerves may have benefits as outlined above, there are little to no data on outcomes of nerve repair or grafting in ballistic injuries in the more acute setting, 1 to 2 weeks after injury. Further research is needed both with regards to diagnosis and utilization of ultrasound, as well as postoperative outcomes in patients with ballistic nerve injuries to help guide our ever-evolving treatment protocols.
Keywords: Ballistic; Brachial plexus; Gunshot wound; Nerve.
© 2024 The Authors.
Conflict of interest statement
No benefits in any form have been received or will be received related directly to this article.
Figures




References
-
- Omer G.E. Injuries to nerves of the upper extremity. J Bone Joint Surg Am. 1974;56(8):1615–1624. - PubMed
-
- Omer G.E. Results of untreated peripheral nerve injuries. Clin Orthop Relat Res. 1982;163:15–19. - PubMed
-
- Veltre D.R., Tornetta P., Krause P., et al. Gunshot fractures of the forearm: a multicenter evaluation. J Orthop Trauma. 2021;35(10):E364–E370. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
