

Long-term autonomy, professional activities, cognition, and overall survival after awake functional-based surgery in patients with IDH-mutant grade 2 gliomas: a retrospective cohort study
- PMID: 39381547
- PMCID: PMC11458993
- DOI: 10.1016/j.lanepe.2024.101078
Long-term autonomy, professional activities, cognition, and overall survival after awake functional-based surgery in patients with IDH-mutant grade 2 gliomas: a retrospective cohort study
Abstract
Background: In isocitrate dehydrogenase (IDH)-mutant low-grade gliomas (LGGs), awake functional-based resection (i.e., resection based on intraoperative functional responses rather than anatomical margins) has emerged as an efficient method to reduce tumour volume (TV) while minimizing postoperative deficits. Here, our goal was to assess the long-term onco-functional outcomes after awake functional-based resection in IDH-mutant LGGs, in conjunction with clinico-radiological and molecular factors.
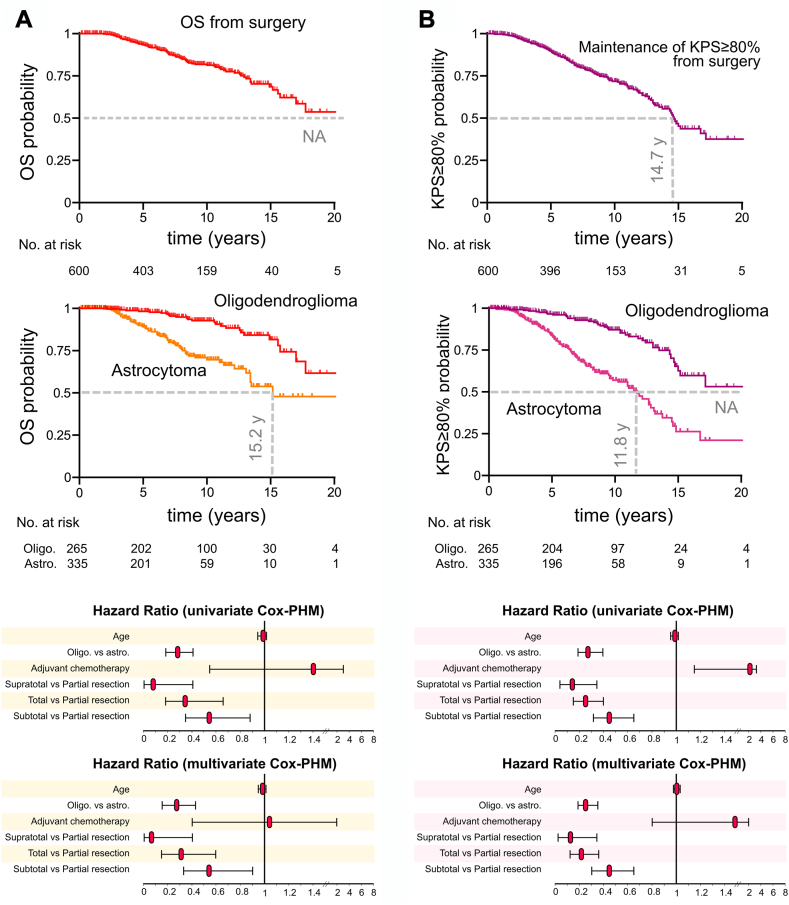
Methods: We retrospectively studied a consecutive cohort (June 1997-January 2023) of 949 patients. Six hundred patients with IDH-mutant LGGs benefited from an awake functional-based resection with a median follow-up of 7.8 years (95% Confidence interval [CI]: 7.1-8.4 years). The main outcomes were the overall survival (OS), the OS with Karnofsky performance status ≥80% (OSKPS ≥ 80%), cognition measures, and professional activities at 12 months post-surgery.
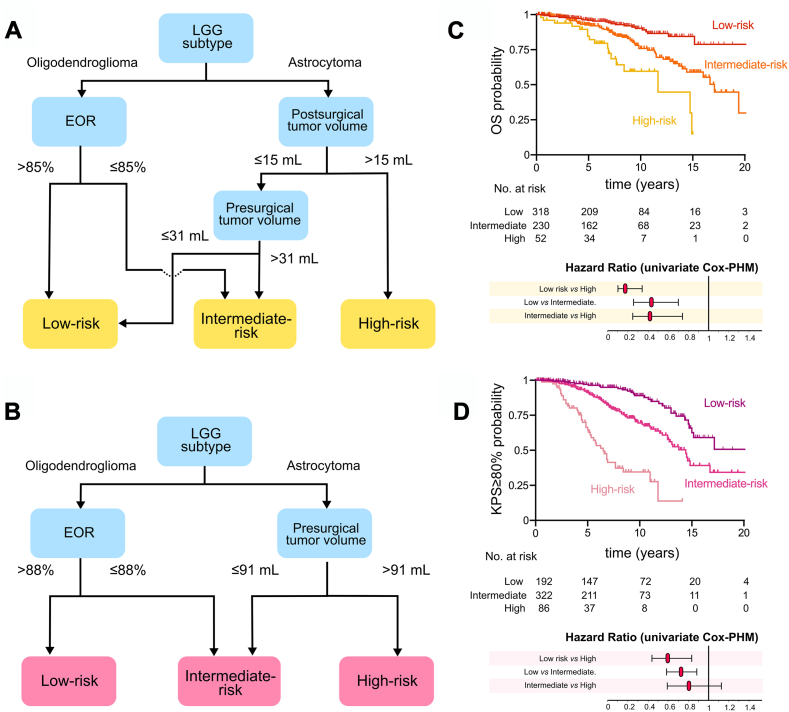
Findings: 600 patients were included in the cohort (274 female [46.0%], median age: 36 years [Interquartile range, IQR: 30-44 years]). The rate of return to work was 93.7%. The impact of surgery on cognition was of limited magnitude. The median postsurgical TV of 2.5 mL (IQR: 0-8.0 mL). The median OS was over 20 years (median: NA, 95% CI: 17.0-NA years). The median OSKPS ≥ 80% was 14.7 years (95% CI: 13.2-17.2 years). Factors associated with longer OS and OSKPS ≥ P80% were 1p19q codeletion (Hazard ratio [HR]OS: 0.27, 95% CI: 0.16-0.43, HRKPS ≥ 80%:0.25, 95% CI: 0.17-0.36), supratotal resection (HROS: 0.08, 95% CI: 0.005-0.40, HRKPS ≥ 80%:0.12, 95% CI: 0.03-0.34) and total resection (HROS: 0.31, 95% CI: 0.16-0.59, HRKPS ≥ 80%:0.21, 95% CI: 0.12-0.36). Recursive partitioning analyses established three OS and OSKPS ≥ 80% prognostic groups, highlighting the contributions of histomolecular status, extent of resection, postsurgical and presurgical TV. Further propensity-matching analyses confirmed the oncological benefits of supratotal resections.
Interpretation: Awake functional-based resection surgery in newly diagnosed IDH-mutant grade 2 LGG, was an effective strategy associated with long survival (median OS over 20 years) and long-term preservation of autonomy. More complete tumor resections favored better onco-functional outcomes across all molecularly-defined subtypes. Short-term effects were of limited magnitude regarding postoperative cognitive and professional outcomes. Supratotal functional-based resections offered additional survival benefits.
Funding: None.
Keywords: Awake surgery; Functional outcomes; Survival; WHO grade 2 gliomas.
© 2024 The Author(s).
Conflict of interest statement
All authors declare no relevant conflict of interests.
Figures


References
-
- Jakola A.S., Myrmel K.S., Kloster R., et al. Comparison of a strategy favoring early surgical resection vs a strategy favoring watchful waiting in low-grade gliomas. JAMA. 2012;308:1881. - PubMed
-
- Alattar A.A., Brandel M.G., Hirshman B.R., et al. Oligodendroglioma resection: a Surveillance, Epidemiology, and End Results (SEER) analysis. J Neurosurg. 2018;128:1076–1083. - PubMed
LinkOut - more resources
Full Text Sources
