

Future needs for continuing innovation in hemophilia: improving outcomes for individuals of all severities, including women and those in resource-constrained regions
- PMID: 39381602
- PMCID: PMC11459663
- DOI: 10.1177/20406207241285143
Future needs for continuing innovation in hemophilia: improving outcomes for individuals of all severities, including women and those in resource-constrained regions
Abstract
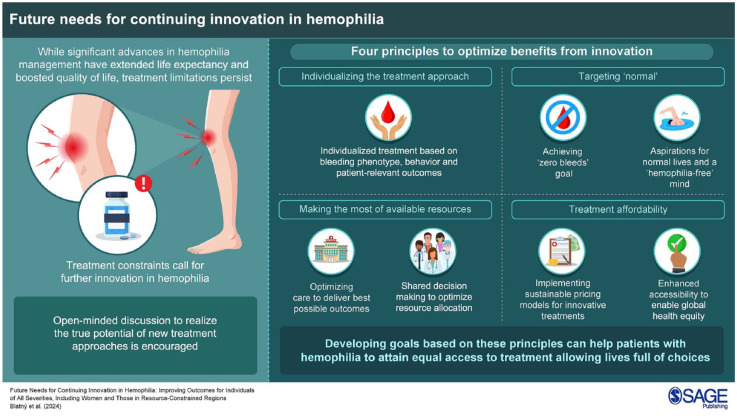
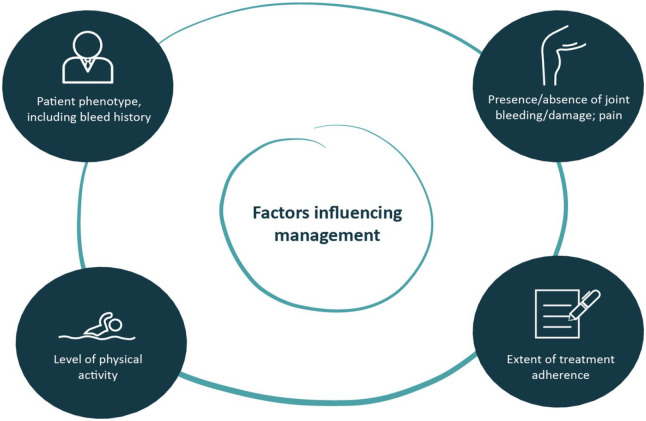
Over recent decades, management of people with hemophilia (PwH) has been greatly improved by scientific advances that have resulted in a rich and varied therapeutic landscape. Nevertheless, treatment limitations continue to drive innovation, and emerging options have the potential to realize further improvement. We advocate four general principles to optimize benefits from innovation: individualizing the treatment approach, targeting 'normal,' making the most of available resources, and considering treatment affordability. Ultimately, all PwH-men and women, of all ages and severities, and worldwide-should have access to treatment that fully prevents bleeding, while allowing personal, social, family, and professional lives of choice. Clearly, we are not there yet, but developing goals/milestones based on the principles we describe may help to achieve this.
Keywords: hemophilia; innovation; management; outcomes; quality of life.
© The Author(s), 2024.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JB has received consultation and/or speaker’s fees from NovoNordisk, Roche, Sobi, Takeda, and CSL Behring. JA has received research grants from Sobi, CSL Behring, Takeda/Shire, and Bayer, and speaker’s fees and consultancy for Octapharma, Novo Nordisk, Pfizer, Bayer, Sobi, CSL Behring, Takeda/Shire, BioMarin, Uniqure, and Spark Therapeutics. CC has received payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events, and support for attending meetings and/or travel from Sobi, Bayer, Roche, and Novo Nordisk, and has also participated in data safety monitoring boards or advisory boards for Sobi, Bayer, Roche, and Novo Nordisk. GD has received consulting fees from Pfizer, Biomarin, CSL, Roche, and Sobi, and payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events from Pfizer, Spark Therapeutics, CSL, Bayer, Takeda, Roche, Chugai, and Sobi. KF has received unrestricted research grants from CSL Behring, Sobi, and Novo Nordisk, as well as consultancy fees from Hoffman-La Roche, Sanofi, Sobi, and Novo Nordisk, with all fees paid to her institution. CH has received research funding from Bayer, BioMarin, CSL Behring, Novo Nordisk, Pfizer, Shire/Takeda, and Sobi, as well as honoraria/speaker’s bureau fees from Bayer, CAF-DCF, CSL Behring, Hoffmann-La Roche, LFB, Novo Nordisk, Octapharma, Pfizer, Shire/Takeda, Sobi, and UniQure. KH has received grants for research or clinical studies (paid to her institution) from Bayer, CSL Behring, Novo Nordisk, Pfizer, Regeneron, Sanofi, and Sobi, as well honoraria or consultancy fees from Bayer, Biomarin, Biotest, CSL Behring, LFB, Novo Nordisk, Pfizer, Roche, Sobi, and Takeda. VJ-Y has received reimbursement for attending symposia/congresses and/or honoraria for speaking and/or honoraria for consulting, and/or funds for research from Takeda, Bayer, BioMarin, CSL Behring, Grifols, Novo Nordisk, Sobi, Roche, Octapharma, and Pfizer. RK has received consultancy fees and honoraria for lectures and advisory boards from Bayer, Biomarin, CSL Behring, Novo Nordisk, Grifols, Octapharma, Pfizer, Roche/Chugai, Sanofi, Sobi, and Takeda. ML has served on an advisory board for CSL Behring, as a consultant for Sobi, CSL Behring, Takeda, and Band Therapeutics, and has received research funding from Takeda and speaker fees from Sobi and Takeda. PJL has received research support to his institute from Sobi, Sanofi, BioMarin, and Roche. SL has acted as a paid consultant to Faust Pharmaceuticals Inc. MEM has acted as a paid speaker/consultant/advisor for Bayer, Biomarin, CSL Behring, Kedrion, LFB, Octapharma, Novo Nordisk, Pfizer, Roche, Sanofi, Sobi, and Takeda. JM has received honoraria and/or educational support from Sobi, Roche, Bayer, and CSL. JSO’D declares no conflicts of interest beyond the support for this manuscript from Sobi. CK has received funding from BFSH, Bayer, CSL Behring, Florio, MSD, Novo Nordisk, Roche/Chugai, Sobi/Sanofi, and Takeda for presentations and/or scientific advice, and his institution has received research funding from Bayer, Biotest, CSL Behring, Intersero, Novo Nordisk, Pfizer, Roche/Chugai, Sobi/Sanofi, and Takeda.
Figures

References
-
- White GC, II, Rosendaal F, Aledort LM, et al.. Definitions in hemophilia. Recommendation of the Scientific Subcommittee on Factor VIII and Factor IX of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost 2001; 85: 560. - PubMed
-
- Thachil J, Connors JM, Mahlangu J, et al.. Reclassifying hemophilia to include the definition of outcomes and phenotype as new targets. J Thromb Haemost 2023; 21: 1737–1740. - PubMed
-
- Young G, Makris M. Time to revisit the classification of hemophilia: if it ain’t broke, don’t fix it! J Thromb Haemost 2023; 21: 1755–1756. - PubMed
-
- Gorman R, Woollard L. “Reclassifying hemophilia to include the definition of outcomes and phenotype as new targets”: comment. J Thromb Haemost 2023; 21: 2977–2979. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
