

A phase III, open-label clinical trial evaluating pegunigalsidase alfa administered every 4 weeks in adults with Fabry disease previously treated with other enzyme replacement therapies
- PMID: 39381863
- PMCID: PMC11667655
- DOI: 10.1002/jimd.12795
A phase III, open-label clinical trial evaluating pegunigalsidase alfa administered every 4 weeks in adults with Fabry disease previously treated with other enzyme replacement therapies
Abstract
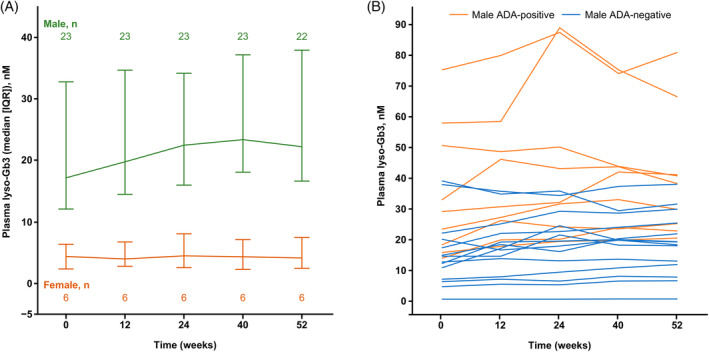
Pegunigalsidase alfa, a PEGylated α-galactosidase A enzyme replacement therapy (ERT) for Fabry disease, has a longer plasma half-life than other ERTs administered intravenously every 2 weeks (E2W). BRIGHT (NCT03180840) was a phase III, open-label study in adults with Fabry disease, previously treated with agalsidase alfa or beta E2W for ≥3 years, who switched to 2 mg/kg pegunigalsidase alfa every 4 weeks (E4W) for 52 weeks. Primary objective assessed safety, including number of treatment-emergent adverse events (TEAEs). Thirty patients were enrolled (24 males); 23 previously received agalsidase beta. Pegunigalsidase alfa plasma concentrations remained above the lower limit of quantification throughout the 4-week dosing interval. Thirty-three of 182 TEAEs (in 9 patients) were considered treatment-related; all were mild/moderate. No patients developed de novo anti-drug antibodies (ADAs). In the efficacy analysis (n = 29), median (inter-quartile range) eGFR change from baseline over 52 weeks was -1.9 (-5.9; 1.8) mL/min/1.73 m2 (n = 28; males [n = 22]: -2.4 [-5.2; 3.2]; females [n = 6]: -0.7 [-9.2; 2.0]). Overall, median eGFR slope was -1.9 (-8.3; 1.9) mL/min/1.73 m2/year (ADA-negative [n = 20]: -1.2 [-6.4; 2.6]; ADA-positive [n = 9]: -8.4 [-11.6; -1.0]). Lyso-Gb3 concentrations were low and stable in females, with a slight increase in males (9/24 ADA-positive). The BRIGHT study results suggest that 2 mg/kg pegunigalsidase alfa E4W is tolerated well in stable adult patients with Fabry disease. Due to the low number of patients in this study, more research is needed to demonstrate the effects of pegunigalsidase alfa given E4W. Further evidence, outside of this clinical trial, should be factored in for physicians to prolong the biweekly ERT intervals to E4W. TAKE-HOME MESSAGE: Treatment with 2 mg/kg pegunigalsidase alfa every 4 weeks could offer a new treatment option for patients with Fabry disease.
Keywords: Fabry disease; eGFR; enzyme replacement therapy; lysosomal storage disorders; lyso‐Gb3; pegunigalsidase alfa.
© 2024 The Author(s). Journal of Inherited Metabolic Disease published by John Wiley & Sons Ltd on behalf of SSIEM.
Conflict of interest statement
AL has received speaker's honoraria and/or consulting fees from Amicus Therapeutics, Chiesi, Protalix Biotherapeutics, Sanofi, and Takeda. AP has received grants and travel support from Amicus, Genzyme/Sanofi, Chiesi, Protalix Biotherapeutics, and Shire. AS was a paid consultant for Chiesi and Protalix Biotherapeutics. CT has received speaker's honoraria and/or consulting fees for advisory board meetings from Acelink, Amicus, Chiesi, Freeline, Sangamo, and Sanofi. DGW has no conflicts of interest to report. DH has received speaker's honoraria and/or consulting fees for advisory board meetings from Amicus, Chiesi, Protalix Biotherapeutics, Freeline, Sangamo, Sanofi, and Takeda. EW has been involved in clinical trials with Spark Therapeutics, Idorsia, Sanofi Genzyme, Protalix Biotherapeutics, and Chiesi. He is also a consultant for Amicus, Chiesi, Protalix Biotherapeutics, Sanofi, and Walking Fish; and has received a research grant from Sanofi. FE has received speaker's fees or honoraria for lectures, presentations, or educational events from Amicus, Sanofi, and Takeda; has received meeting attendance and/or travel support from Recordati, Sanofi, and Takeda; and has been involved in advisory board meetings with Chiesi, Protalix Biotherapeutics, Sanofi, and Ultragenyx. JAB receives research support from Avrobio, BioMarin Pharmaceutical, Chiesi Farmaceutici, Idorsia Pharmaceuticals, Pfizer, Protalix Biotherapeutics, Sangamo Therapeutics, Sanofi, Takeda, and Travere Therapeutics; has received a speaker's honorarium from the Fabry Support and Information Group; and has been involved in advisory board meetings with Chiesi USA, Sanofi, and Takeda. MH was a principal or co‐investigator on the initial phase I–III pegunigalsidase alfa trials. He has also received speaker's honoraria from Chiesi and Protalix Biotherapeutics, and has participated in advisory boards with Sanofi and Amicus. NL has been involved in clinical trials with Aeglea, Amicus, Audentes/Astellas, BioMarin, Chiesi, Protalix Biotherapeutics, Genzyme/Sanofi, Hemoshear, Homology, Horizon Pharma, Moderna, Pfizer, PTC Therapeutics, Reneo, Synlogic, Takeda, Travere Therapeutics, and Ultragenyx; and his Institution has received consulting fees for advisory board meetings from Alnylam, Amicus, Audentes/Astellas, BioMarin, BridgeBio/CoA Therapeutics, Chiesi, Genzyme/Sanofi, Hemoshear, Horizon Pharma, Jaguar Gene Therapy, Jnana, Leadiant Biosciences, Moderna, Nestle’ Pharma, PTC Therapeutics, Recordati, Reneo, Synlogic, Takeda, and Ultragenyx. OGA has received grant support and consultancy fees from Chiesi. PD received institutional support for expenses incurred during the conduct of this trial from Protalix Biotherapeutics, and travel support from Chiesi. SW was a paid consultant for Chiesi and Protalix Biotherapeutics. UFR has received speaker's honoraria and/or consulting fees for advisory board meetings from Amicus, Chiesi, Protalix Biotherapeutics, Freeline, Recordati, Sanofi, and Takeda. UFR's research salary was sponsored by a grant from Kirsten and Freddy Johansen's Fund. WRW has been a consultant for Chiesi, Sanofi Genzyme, Amicus, Takeda, Spark, and UniQure; has been involved in clinical trials with Chiesi, Protalix Biotherapeutics, Sanofi Genzyme, Takeda, Amicus, 4D Molecular Therapeutics, and Sangamo; and has received research grants from Amicus and Takeda. RR is an employee of Chiesi Farmaceutici S.p.A. EBA and RC were full‐time employees of Protalix Biotherapeutics at the time of study conduct and analysis, and are now consultants to Protalix Biotherapeutics. SA is a full‐time employee of Protalix Biotherapeutics.
Figures




References
-
- Mehta A, Hughes DA. Fabry disease. In: Adam MP, Mirzaa GM, Pagon RA, et al., eds. GeneReviews(®). University of Washington; 2002. (updated March 9, 2023).
-
- National Institutes of Health . Fabry disease. 2022. https://medlineplus.gov/genetics/condition/fabry-disease/#frequency Accessed December 12, 2023.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
