

Economic Burden of Community-Acquired Antibiotic-Resistant Urinary Tract Infections: Systematic Review and Meta-Analysis
- PMID: 39382601
- PMCID: PMC11481822
- DOI: 10.2196/53828
Economic Burden of Community-Acquired Antibiotic-Resistant Urinary Tract Infections: Systematic Review and Meta-Analysis
Abstract
Background: Antibiotic resistance (ABR) poses a major burden to global health and economic systems. ABR in community-acquired urinary tract infections (CA-UTIs) has become increasingly prevalent. Accurate estimates of ABR's clinical and economic burden are needed to support medical resource prioritization and cost-effectiveness evaluations of urinary tract infection (UTI) interventions.
Objective: This study aims to systematically synthesize the evidence on the economic costs associated with ABR in CA-UTIs, using published studies comparing the costs of antibiotic-susceptible and antibiotic-resistant cases.
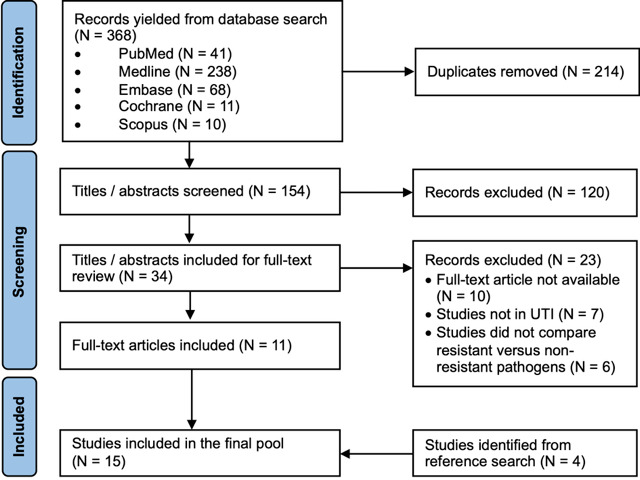
Methods: We searched the PubMed, Ovid MEDLINE and Embase, Cochrane Review Library, and Scopus databases. Studies published in English from January 1, 2008, to January 31, 2023, reporting the economic costs of ABR in CA-UTI of any microbe were included. Independent screening of titles/abstracts and full texts was performed based on prespecified criteria. A quality assessment was performed using the Integrated Quality Criteria for Review of Multiple Study Designs (ICROMS) tool. Data in UTI diagnosis criteria, patient characteristics, perspectives, resource costs, and patient and health economic outcomes, including mortality, hospital length of stay (LOS), and costs, were extracted and analyzed. Monetary costs were converted into 2023 US dollars.
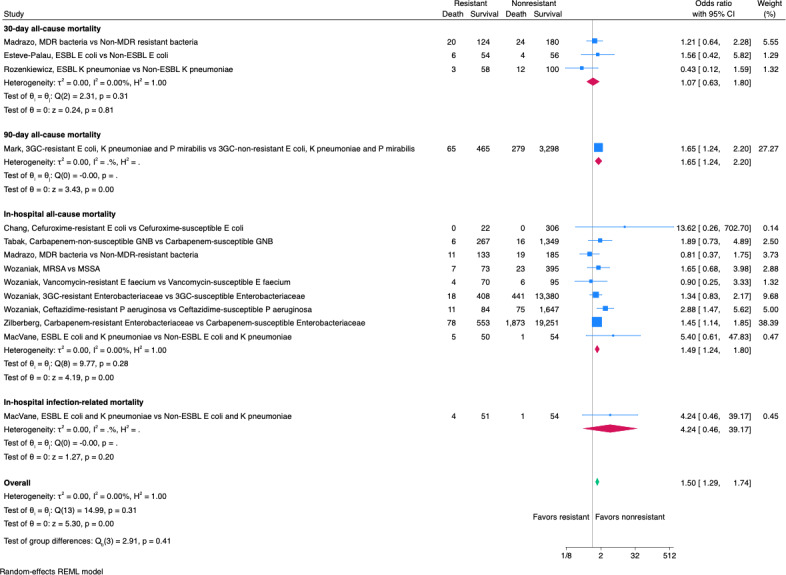
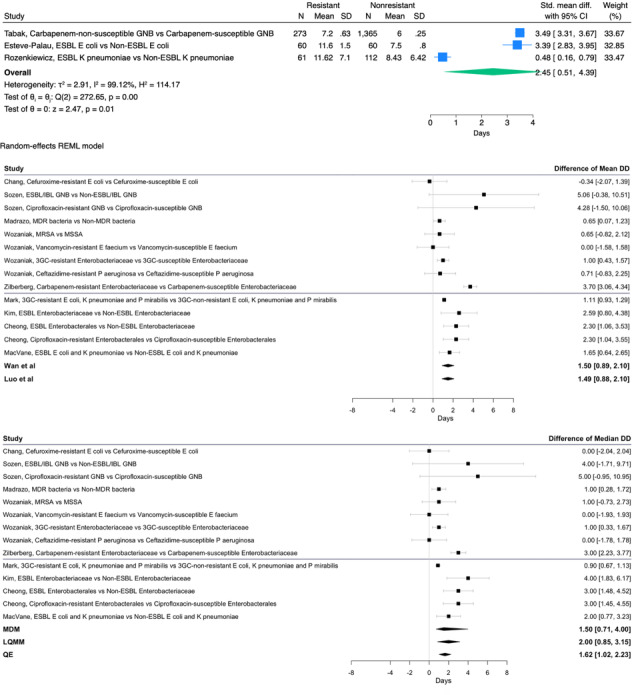
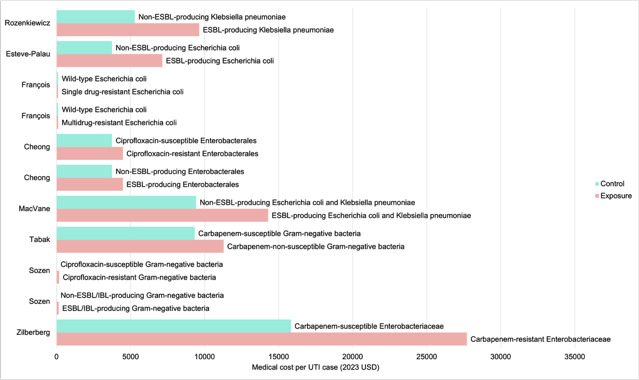
Results: This review included 15 studies with a total of 57,251 CA-UTI cases. All studies were from high- or upper-middle-income countries. A total of 14 (93%) studies took a health system perspective, 13 (87%) focused on hospitalized patients, and 14 (93%) reported UTI pathogens. Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa are the most prevalent organisms. A total of 12 (80%) studies reported mortality, of which, 7 reported increased mortality in the ABR group. Random effects meta-analyses estimated an odds ratio of 1.50 (95% CI 1.29-1.74) in the ABR CA-UTI cases. All 13 hospital-based studies reported LOS, of which, 11 reported significantly higher LOS in the ABR group. The meta-analysis of the reported median LOS estimated a pooled excess LOS ranging from 1.50 days (95% CI 0.71-4.00) to 2.00 days (95% CI 0.85-3.15). The meta-analysis of the reported mean LOS estimated a pooled excess LOS of 2.45 days (95% CI 0.51-4.39). A total of 8 (53%) studies reported costs in monetary terms-none discounted the costs. All 8 studies reported higher medical costs spent treating patients with ABR CA-UTI in hospitals. The highest excess cost was observed in UTIs caused by carbapenem-resistant Enterobacterales. No meta-analysis was performed for monetary costs due to heterogeneity.
Conclusions: ABR was attributed to increased mortality, hospital LOS, and economic costs among patients with CA-UTI. The findings of this review highlighted the scarcity of research in this area, particularly in patient morbidity and chronic sequelae and costs incurred in community health care. Future research calls for a cost-of-illness analysis of infections, standardizing therapy-pathogen combination comparators, medical resources, productivity loss, intangible costs to be captured, and data from community sectors and low-resource settings and countries.
Keywords: antibiotic resistance; cost-effectiveness; hospital length of stay; mortality; urinary tract infection.
© Nina Jiayue Zhu, Misghina Weldegiorgis, Emma Carter, Colin Brown, Alison Holmes, Paul Aylin. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org).
Conflict of interest statement
Figures
References
-
- Urinary tract infection (lower) - women. Clinical knowledge summaries (CKS) National Institute for Health and Care Excellence. [14-10-2023]. https://cks.nice.org.uk/topics/urinary-tract-infection-lower-women/ URL. Accessed.
-
- Gharbi M, Drysdale JH, Lishman H, et al. Antibiotic management of urinary tract infection in elderly patients in primary care and its association with bloodstream infections and all cause mortality: population based cohort study. BMJ. 2019 Feb 27;364:l525. doi: 10.1136/bmj.l525. doi. Medline. - DOI - PMC - PubMed
-
- Shallcross L, Rockenschaub P, Blackburn R, Nazareth I, Freemantle N, Hayward A. Antibiotic prescribing for lower UTI in elderly patients in primary care and risk of bloodstream infection: a cohort study using electronic health records in England. PLoS Med. 2020 Sep 21;17(9):e1003336. doi: 10.1371/journal.pmed.1003336. doi. Medline. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
