

[Volume therapy: which preparation for which situation?]
- PMID: 39382683
- PMCID: PMC11538216
- DOI: 10.1007/s00063-024-01194-0
[Volume therapy: which preparation for which situation?]
Abstract
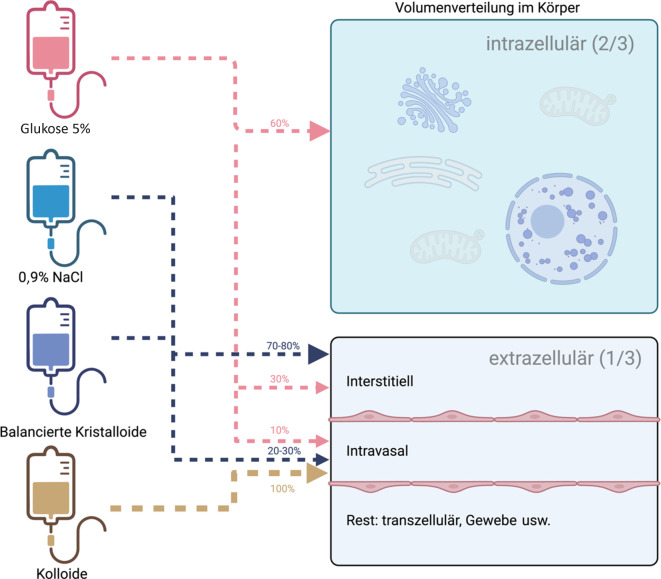
The most commonly used fluids for volume therapy are crystalloids and colloids. Crystalloids comprise 0.9% sodium chloride and balanced crystalloids (BC). Colloids can be divided into artificial colloids and human albumin (a natural colloid). Large studies show advantages for BC over 0.9% NaCl with respect to renal endpoints, probably due to the unphysiologically high chloride content of 0.9% NaCl. However, other studies, such as the BaSICS and PLUS trials, showed no significant differences in mortality in a heterogeneous population. Despite this, meta-analyses suggest advantages for BC. Therefore, BC should be preferred, especially in patients at increased risk of acute kidney injury, with acidemia and/or hyperchloremia. Except for specific indications (e.g., in patients with cirrhosis, sepsis resuscitation after initial volume therapy with BC), albumin should not be used. There is clear evidence of harm from hydroxyethyl starch in intensive care patients.
Die gängigen zur Volumentherapie verwendeten Lösungen sind Kristalloide und Kolloide. Kristalloide lassen sich in 0,9 % Natriumchlorid (NaCl) und balancierte Kristalloide (BK) unterteilen. Kolloide können in künstliche/artifizielle Kolloide und Humanalbumin (als natürliches Kolloid) unterteilt werden. Große Studien konnten Vorteile von BK gegenüber 0,9 % NaCl in Bezug auf renale Endpunkte zeigen, was vor allem durch den unphysiologisch hohen Chloridgehalt in 0,9 % NaCl bedingt sein dürfte. Weitere Studien wie BaSICS und PLUS Trial zeigten an einem heterogenen Kollektiv keine signifikanten Unterschiede in der Mortalität. Jedoch deuten Metaanalysen auf Vorteile der BK hin. Insbesondere bei Patient:innen mit erhöhtem Risiko für eine akute Nierenschädigung, Azidose und/oder Hyperchlorämie sollten daher primär BK verwendet werden. Außer für spezielle Indikationen, so etwa bei Patient:innen mit Leberzirrhose oder „resuscitation“ in der Sepsis nach initialer Volumentherapie mit BK, sollte Albumin nicht eingesetzt werden. Andere, artifizielle, Kolloide sollten mit Zurückhaltung verabreicht werden. Für Hydroxyethylstärke gibt es eindeutige Schädigungssignale bei Intensivpatient:innen.
Keywords: Colloids; Crystalloid solutions, balanced; Normal saline solution; Sepsis; Serum albumin, human.
© 2024. The Author(s).
Figures

References
-
- Woodcock T (2024) Fluid Physiology Part 1: Volume and Distribution of Water and Its Major Solutes Between Plasma, the Interstitium and Intracellular Fluid. In: Malbrain MLNG, Wong A, Nasa P, Ghosh S (Hrsg) Rational Use of Intravenous Fluids in Critically Ill Patients. Springer, Cham, S 47–74 10.1007/978-3-031-42205-8_2
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
