

Association between delta anion gap/delta bicarbonate and outcome of surgical patients admitted to intensive care unit
- PMID: 39385064
- PMCID: PMC11463135
- DOI: 10.1186/s12871-024-02564-z
Association between delta anion gap/delta bicarbonate and outcome of surgical patients admitted to intensive care unit
Abstract
Background: Patients undergoing high-risk surgeries with acid-based disorders are associated with poor outcomes. The screening of mixed acid-based metabolic disorders by calculating delta anion gap (AG)/delta bicarbonate (Bic) has a clinically relevant role in patients with high AG metabolic acidosis (MA), however its utility in individuals facing high-risk surgical procedures remains unclear.
Objective: Characterize metabolic acidosis using delta-AG/delta-Bic and its associations in patients undergoing high-risk surgeries with possible outcome-related complications.
Design: Prospective observational multicentric study.
Setting: Three tertiary hospitals in Brazil.
Patients: Patients undergoing high-risk surgeries, aged 18 years or older, requiring postoperative critical care.
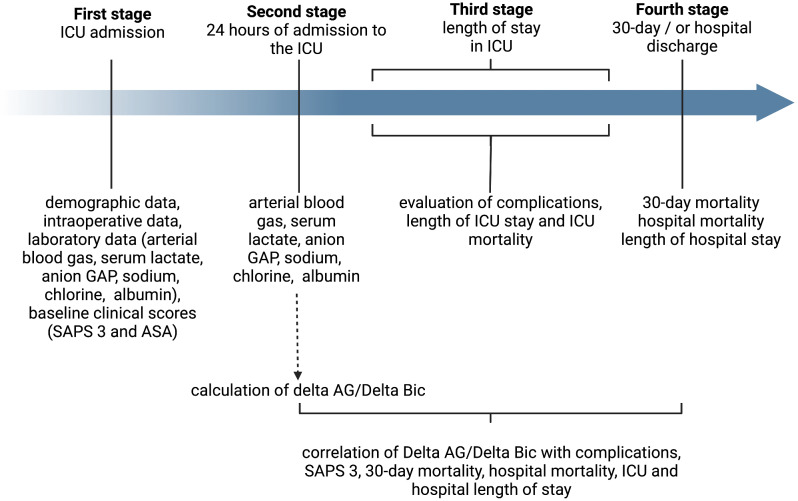
Main outcome measures: Patients undergoing high-risk surgeries monitored during the postoperative phase across three distinct intensive care units (ICUs), with assessment encompassing laboratory analyses upon admission and 24 h thereafter. Patients with MA and with elevated AG within 24 h were separated into 3 subgroups: [G1 - delta-AG/delta-Bic < 1.0] MA associated with hyperchloremia; [G2 - delta-AG/delta-Bic between 1.0 and 1.6] MA and no mixed disorders; and [G3 - delta-AG/delta-Bic > 1.6] MA associated with alkalosis. Primary endpoint was 30-day mortality. The secondary endpoints were cardiovascular, respiratory, renal, neurological, coagulation and infective complications.
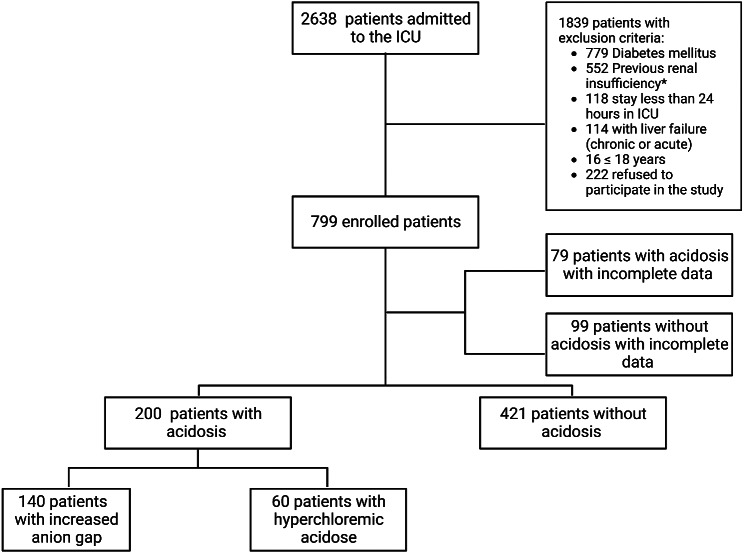
Results: From the 621 surgical patients admitted to ICU, 421 (51.7%) had any type of acidosis. After 24 h, 140 patients remained with MA with elevated AG (G1: 101, G2: 18, and G3: 21). When compared to patients from subgroups 1 and 3, the subgroup with no mixed disorders 2 showed higher 30-day mortality (adjusted HR = 3.72; 95% CI 1.11-12.89, p = 0.001), cardiovascular complications (p = 0.001), ICU mortality (p = 0.03) and sum of all complications during the ICU period (p = 0.021).
Conclusion: In the postoperative time, patients with metabolic acidosis and no mixed disorders present higher ICU-Mortality and higher cardiovascular postoperative complications when compared with patients with combined hyperchloremia or alkalosis. Delta-AG/delta-Bic can be a useful tool to evaluate major clinical outcomes in this population.
Keywords: Anion gap; Critical care; Intensive care; Metabolic acidosis; Surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Silva JM, Oliveira AM, Marti YN, Gonzaga TB, Ferreira AMP, Maia V, Rezend E. Outcome of surgical patients who present acidosis postoperatively. Crit Care. 2011;15(2):P64.
-
- Silva JM Jr., Ribas Rosa de Oliveira, Mendes Nogueira AM, Vianna FA, Amendola PM, Carvalho Carmona CP, LM SM MJ. Metabolic Acidosis Assessment in High-Risk surgeries: Prognostic Importance. Anesth Analg. 2016;123(5):1163–71. - PubMed
-
- Oh TK, Do SH, Jeon YT, Kim J, Na HS, Hwang JW. Association of Preoperative Serum Chloride levels with mortality and morbidity after noncardiac surgery: a retrospective cohort study. Anesth Analg. 2019;129(6):1494–501. - PubMed
-
- McCluskey SA, Karkouti K, Wijeysundera D, Minkovich L, Tait G, Beattie WS. Hyperchloremia after noncardiac surgery is independently associated with increased morbidity and mortality: a propensity-matched cohort study. Anesth Analg. 2013;117(2):412–21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
