

Tensions between end-of-life care and organ donation in controlled donation after circulatory death: ICU healthcare professionals experiences
- PMID: 39385217
- PMCID: PMC11462860
- DOI: 10.1186/s12910-024-01093-1
Tensions between end-of-life care and organ donation in controlled donation after circulatory death: ICU healthcare professionals experiences
Abstract
Background: The development of controlled donation after circulatory death (cDCD) is both important and challenging. The tension between end-of-life care and organ donation raises significant ethical issues for healthcare professionals in the intensive care unit (ICU). The aim of this prospective, multicenter, observational study is to better understand ICU physicians' and nurses' experiences with cDCD.
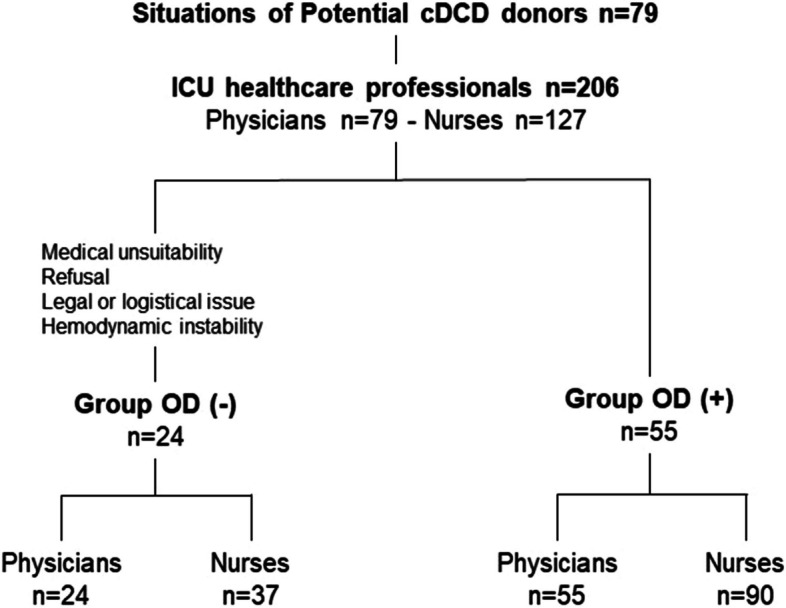
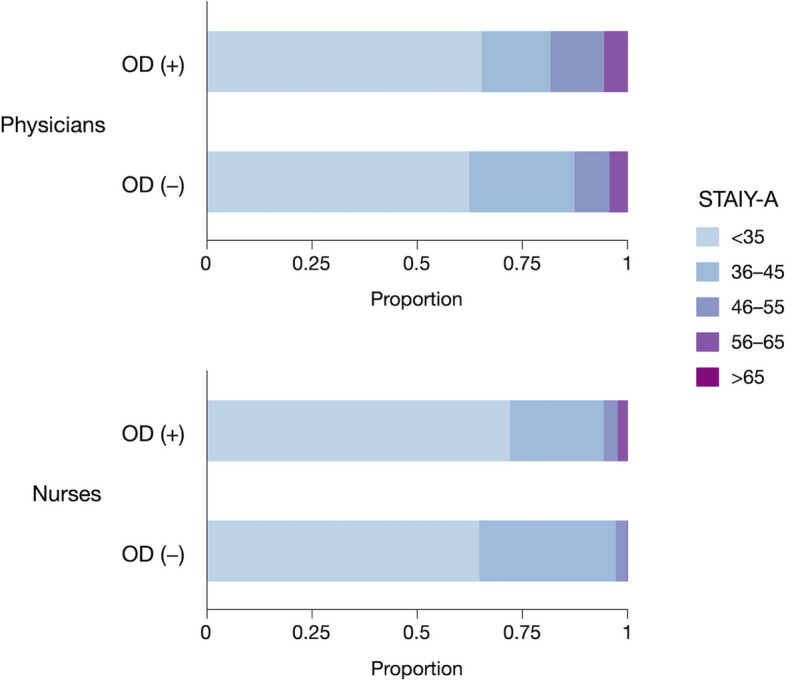
Methods: In 32 ICUs in France, ICU physicians and nurses were invited to complete a questionnaire after the death of end-of-life ICU patients identified as potential cDCD donors who had either experienced the withdrawal of life-sustaining therapies alone or with planned organ donation (OD(-) and OD( +) groups). The primary objective was to assess their anxiety (State Anxiety Inventory STAI Y-A) following the death of a potential cDCD donor. Secondary objectives were to explore potential tensions experienced between end-of-life care and organ donation.
Results: Two hundred six ICU healthcare professionals (79 physicians and 127 nurses) were included in the course of 79 potential cDCD donor situations. STAI Y-A did not differ between the OD(-) and OD( +) groups for either physicians or nurses (STAI Y-A were 34 (27-38) in OD(-) vs. 32 (27-40) in OD( +), p = 0.911, for physicians and 32 (25-37) in OD(-) vs. 39 (26-37) in OD( +), p = 0.875, for nurses). The possibility of organ donation was a factor influencing the WLST decision for nurses only, and a factor influencing the WLST implementation for both nurses and physicians. cDCD experience is perceived positively by ICU healthcare professionals overall.
Conclusions: cDCD does not increase anxiety in ICU healthcare professionals compared to other situations of WLST. WLST and cDCD procedures could further be improved by supporting professionals in making their intentions clear between end-of-life support and the success of organ donation, and when needed, by enhancing communication between ICU physician and nurses.
Trial registration: This research was registered in ClinicalTrials.gov (Identifier: NCT05041023, September 10, 2021).
Keywords: Controlled donation after circulatory death; End-of-life care; Intensive Care Units; Organ donation; Withdrawal of life sustaining therapies.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Savoye E, Legeai C, Branchereau J, Gay S, Riou B, Gaudez F, et al. Optimal donation of kidney transplants after controlled circulatory death. Am J Transplant. 2021;21(7):2424–36. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
