

Building a machine learning-assisted echocardiography prediction tool for children at risk for cancer therapy-related cardiomyopathy
- PMID: 39385257
- PMCID: PMC11462765
- DOI: 10.1186/s40959-024-00268-4
Building a machine learning-assisted echocardiography prediction tool for children at risk for cancer therapy-related cardiomyopathy
Abstract
Background: Despite routine echocardiographic surveillance for childhood cancer survivors, the ability to predict cardiomyopathy risk in individual patients is limited. We explored the feasibility and optimal processes for machine learning-enhanced cardiomyopathy prediction in survivors using serial echocardiograms from five centers.
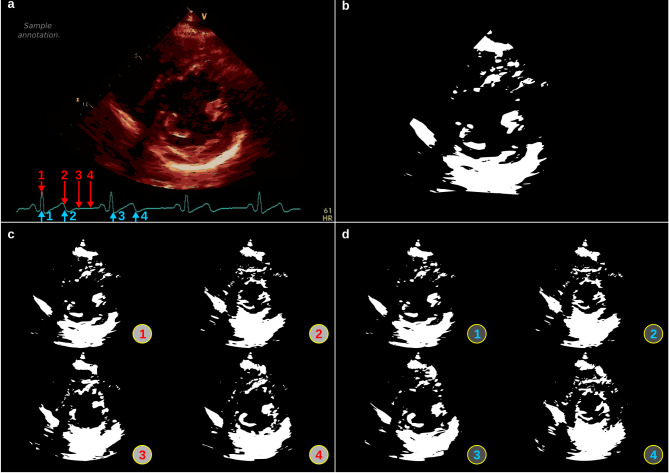
Methods: We designed a series of deep convolutional neural networks (DCNNs) for prediction of cardiomyopathy (shortening fraction ≤ 28% or ejection fraction ≤ 50% on two occasions) for at-risk survivors ≥ 1-year post initial cancer therapy. We built DCNNs with four subsets of echocardiographic data differing in timing relative to case (survivor who developed cardiomyopathy) index diagnosis and two input formats (montages) with differing image selections. We used holdout subsets in a 10-fold cross-validation framework and standard metrics to assess model performance (e.g., F1-score, area under the precision-recall curve [AUPRC]). Performance of the input formats was compared using a combined 5 × 2 cross-validation F-test.
Results: The dataset included 542 pairs of montages: 171 montage pairs from 45 cases at time of cardiomyopathy diagnosis or pre-diagnosis and 371 pairs from 70 at-risk survivors who didn't develop cardiomyopathy during follow-up (non-case). The DCNN trained to distinguish between non-case and time of cardiomyopathy diagnosis or pre-diagnosis case montages achieved an AUROC of 0.89 ± 0.02, AUPRC 0.83 ± 0.03, and F1-score: 0.76 ± 0.04. When limited to smaller subsets of case data (e.g., ≥ 1 or 2 years pre-diagnosis), performance worsened. Model input format did not impact performance accuracy across models.
Conclusions: This methodology is a promising first step toward development of a DCNN capable of accurately differentiating pre-diagnosis versus non-case echocardiograms to predict survivors more likely to develop cardiomyopathy.
Keywords: Cancer survivorship; Cardiomyopathy; Echocardiography; Machine learning.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation. 2013;128:1927–95. - PubMed
-
- Cardinale D, Colombo A, Lamantia G, Colombo N, Civelli M, De Giacomi G, et al. Anthracycline-induced cardiomyopathy: clinical relevance and response to pharmacologic therapy. J Am Coll Cardiol. 2010;55:213–20. - PubMed
-
- Investigators SOLVD, Yusuf S, Pitt B, Davis CE, Hood WB, Cohn JN. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med. 1992;327:685–91. - PubMed
-
- Pfeffer MA, Braunwald E, Moyé LA, Basta L, Brown EJ, Cuddy TE, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE investigators. N Engl J Med. 1992;327:669–77. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources