

Optimizing range of motion in reverse shoulder arthroplasty
- PMID: 39385553
- PMCID: PMC11464925
- DOI: 10.1302/2633-1462.510.BJO-2024-0097.R1
Optimizing range of motion in reverse shoulder arthroplasty
Abstract
Aims: Optimal glenoid positioning in reverse shoulder arthroplasty (RSA) is crucial to provide impingement-free range of motion (ROM). Lateralization and inclination correction are not yet systematically used. Using planning software, we simulated the most used glenoid implant positions. The primary goal was to determine the configuration that delivers the best theoretical impingement-free ROM.
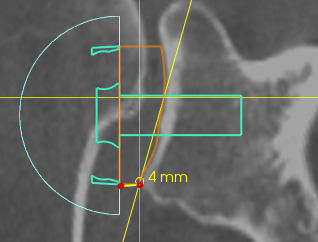
Methods: With the use of a 3D planning software (Blueprint) for RSA, 41 shoulders in 41 consecutive patients (17 males and 24 females; means age 73 years (SD 7)) undergoing RSA were planned. For the same anteroposterior positioning and retroversion of the glenoid implant, four different glenoid baseplate configurations were used on each shoulder to compare ROM: 1) no correction of the RSA angle and no lateralization (C-L-); 2) correction of the RSA angle with medialization by inferior reaming (C+M+); 3) correction of the RSA angle without lateralization by superior compensation (C+L-); and 4) correction of the RSA angle and additional lateralization (C+L+). The same humeral inlay implant and positioning were used on the humeral side for the four different glenoid configurations with a 3 mm symmetric 135° inclined polyethylene liner.
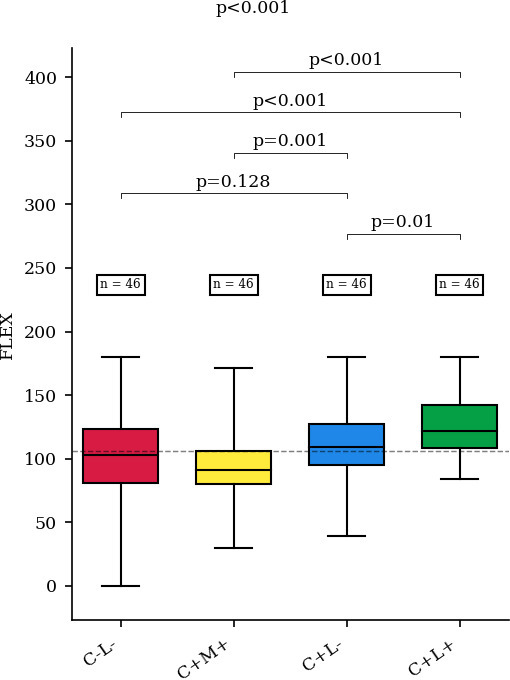
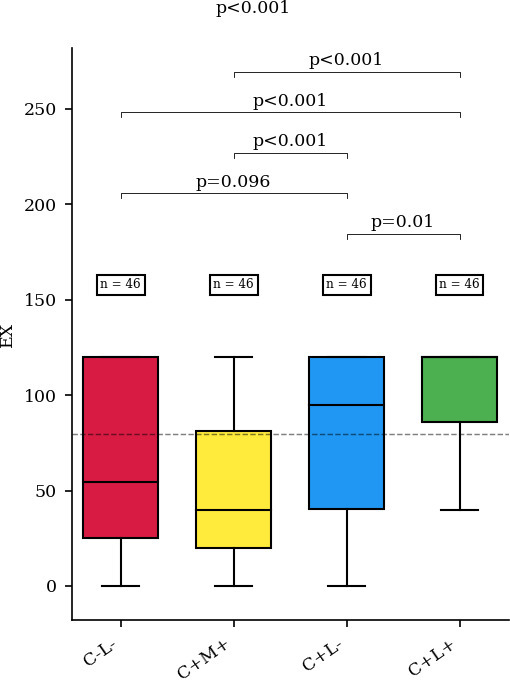
Results: The configuration with lateralization and correction of the RSA angle (C+L+) led to better ROM in flexion, extension, adduction, and external rotation (p ≤ 0.001). Only internal rotation was not significantly different between groups (p = 0.388). The configuration where correction of the inclination was done by medialization (C+M+) led to the worst ROM in adduction, extension, abduction, flexion, and external rotation of the shoulder.
Conclusion: Our software study shows that, when using a 135° inlay reversed humeral implant, correcting glenoid inclination (RSA angle 0°) and lateralizing the glenoid component by using an angled bony or metallic augment of 8 to 10 mm provides optimal impingement-free ROM.
© 2024 Mouchantaf et al.
Conflict of interest statement
P. Boileau reports the conception, and being the developer, of Blueprint software; and receiving royalties from Stryker and Depuy, We used the Bluprint software which is related to this work. M. Chelli discloses being the developer of EasyMedStat, which is also related to this manuscript.
Figures







References
LinkOut - more resources
Full Text Sources
