

The Effect of COVID-19 on Lung Cancer Screening
- PMID: 39385861
- PMCID: PMC11463903
- DOI: 10.7759/cureus.68986
The Effect of COVID-19 on Lung Cancer Screening
Abstract
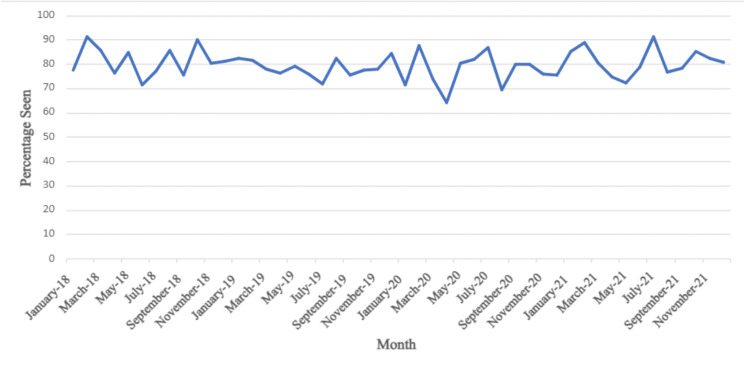
Background During the COVID-19 pandemic, many hospitals suspended non-essential medical procedures to reduce transmission and prioritize personal protective equipment (PPE) for COVID-19 patients. Hospitals that continued these procedures faced uncertainty about patient attendance. Multiple factors could explain a decline in patient attendance during the pandemic, including patients' reluctance to risk COVID-19 exposure in the hospital or their own illness requiring self-isolation. This study aimed to compare attendance rates of lung cancer screenings (LCS) before and during the pandemic. Unlike previous studies conducted on this research topic, the current study documents that the John B. Amos Cancer Center continued LCS throughout the pandemic. The alternative hypothesis was that there would be a decrease in the percentage of LCS performed during the pandemic period due to fear of nosocomial transmission. Materials and methods Data for 2,582 scheduled LCS were retrospectively analyzed on Microsoft Excel 2022 (Microsoft Corporation, Redmond, Washington) from 2018 to 2021. For analysis purposes, 2018 and 2019 were considered pre-COVID years, while 2020 and 2021 were considered COVID years. The average percentage attended was calculated for each year and the standard deviation of that year's percentage. The percentage of patients seen each month was averaged during pre-COVID and COVID years. The p-value was calculated by comparing the average attendance percentage for each month in the pre-COVID and COVID years. A p-value <0.05 was considered significant. Results From 2018 to 2021, over 300 more people were scheduled during the COVID years. Although the percentage seen remained consistent throughout the years, there was an increase in both patients scheduled and seen. The results revealed an insignificant difference in LCS attendance between pre-COVID and COVID years, confirming the importance of their continuation. Conclusion The alternative hypothesis was rejected due to no significant difference in attendance percentage between the pre-COVID and COVID years. Further direction of this study may include monitoring the trend of LCS attendance during post-pandemic years as the transmission rates continue to change.
Keywords: cancer screening; coronavirus; covid-19; lcs; ldct; low-dose computed tomography; lung cancer; nosocomial infection; pandemic; preventative medicine.
Copyright © 2024, Thiruppathi et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Cancer statistics, 2024. Siegel RL, Giaquinto AN, Jemal A. CA Cancer J Clin. 2024;74:12–49. - PubMed
-
- Lung cancer mortality reduction by LDCT screening—results from the randomized German LUSI trial. Becker N, Motsch E, Trotter A, et al. Int J Cancer. 2020;146:1503–1513. - PubMed
-
- Lung cancer: diagnosis and management. Collins LG, Haines C, Perkel R, Enck RE. https://pubmed.ncbi.nlm.nih.gov/17225705/ Am Fam Physician. 2007;75:56–63. - PubMed
LinkOut - more resources
Full Text Sources