

Optimal Sequence for Total Neoadjuvant Therapy in Locally Advanced Rectal Cancer: An Evidence-Based Review
- PMID: 39387519
- PMCID: PMC11465286
- DOI: 10.1002/cam4.70291
Optimal Sequence for Total Neoadjuvant Therapy in Locally Advanced Rectal Cancer: An Evidence-Based Review
Abstract
Introduction: Historically, multimodal therapeutic strategies involving preoperative chemoradiotherapy (CRT), surgery, and adjuvant chemotherapy (CT) have been employed to treat locally advanced rectal cancer (LARC). Total Neoadjuvant Therapy (TNT) is showing promise in improving outcomes. Despite its benefits, the optimal sequencing within TNT-whether induction chemotherapy should precede or follow chemoradiotherapy-remains a critical question. This study endeavors to explore the effects of different TNT sequencing strategies on patient outcomes, including tumor downstaging, pathological response, organ preservation, and the balance between efficacy and tolerability.
Methods: Our methodology entailed a comprehensive literature review conducted on Medline, focusing on recent research, including retrospective studies, systematic reviews, and clinical trials. The review emphasized the comparison of induction chemotherapy versus consolidation chemotherapy within TNT regimens, assessing outcomes such as pathological response, organ preservation rates, and adverse effects. To ensure the selection of appropriate and high-quality studies, specific inclusion and exclusion criteria were applied.
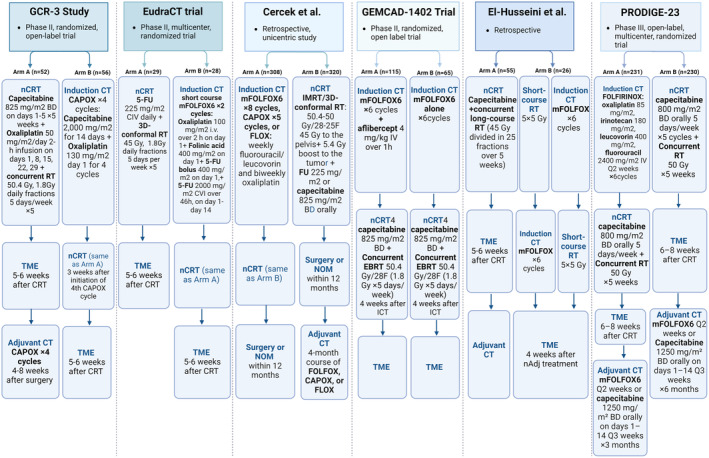
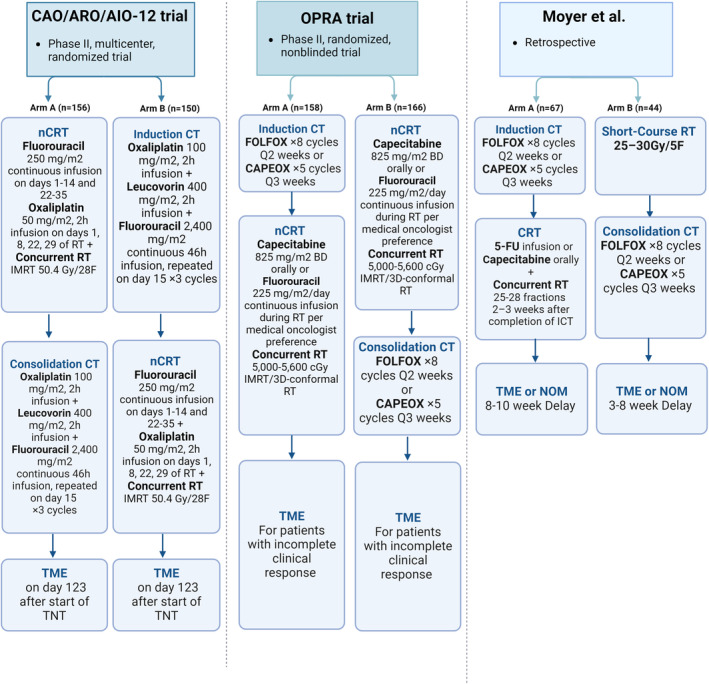
Results: The analysis revealed that induction chemotherapy might lead to decreased adherence to subsequent chemoradiotherapy while offering an early intervention against micrometastasis and potentially improving overall chemotherapy compliance. Conversely, consolidation chemotherapy has been associated with higher pathological complete response (pCR) rates and improved tolerability, indicating its potential for patients requiring local symptom relief or those eligible for a nonoperative management approach. Comparative studies like CAO/ARO/AIO-12 and the OPRA trials have significantly contributed to our understanding, suggesting that while both strategies have distinct advantages, the choice between induction and consolidation chemotherapy should be tailored based on individual patient profiles and tumor characteristics.
Conclusion: This narrative review underscores the importance of a nuanced approach to TNT sequencing in locally advanced rectal cancer, highlighting the need for further research to refine treatment strategies.
Keywords: adenocarcinoma; chemotherapy; radiotherapy; rectal cancer; total neoadjuvant therapy.
© 2024 The Author(s). Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Chemoradiotherapy plus induction or consolidation chemotherapy as total neoadjuvant therapy for locally advanced rectal cancer: Pooled analysis of the CAO/ARO/AIO-12 and the OPRA randomized phase 2 trials.Eur J Cancer. 2024 Oct;210:114291. doi: 10.1016/j.ejca.2024.114291. Epub 2024 Aug 22. Eur J Cancer. 2024. PMID: 39180940 Clinical Trial.
-
Organ Preservation in Rectal Adenocarcinoma: a phase II randomized controlled trial evaluating 3-year disease-free survival in patients with locally advanced rectal cancer treated with chemoradiation plus induction or consolidation chemotherapy, and total mesorectal excision or nonoperative management.BMC Cancer. 2015 Oct 23;15:767. doi: 10.1186/s12885-015-1632-z. BMC Cancer. 2015. PMID: 26497495 Free PMC article. Clinical Trial.
-
[Analysis on efficacy and safety of total neoadjuvant therapy in patients with locally advanced rectal cancer with high risk factors].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Apr 25;22(4):349-356. doi: 10.3760/cma.j.issn.1671-0274.2019.04.007. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31054549 Chinese.
-
Total Neoadjuvant Therapy vs Standard Therapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Dec 1;3(12):e2030097. doi: 10.1001/jamanetworkopen.2020.30097. JAMA Netw Open. 2020. PMID: 33326026 Free PMC article.
-
The Evolving Neoadjuvant Treatment Paradigm for Patients with Locoregional mismatch Repair Proficient Rectal Cancer.Curr Treat Options Oncol. 2022 Apr;23(4):453-473. doi: 10.1007/s11864-022-00961-5. Epub 2022 Mar 21. Curr Treat Options Oncol. 2022. PMID: 35312962 Review.
Cited by
-
CD8-positive lymphocyte infiltration as a marker of anti-tumor immune response in rectal cancer: pre- and post-neoadjuvant radiotherapy comparison.Clin Transl Radiat Oncol. 2025 Jul 16;54:101018. doi: 10.1016/j.ctro.2025.101018. eCollection 2025 Sep. Clin Transl Radiat Oncol. 2025. PMID: 40741211 Free PMC article.
-
Postoperative NEOadjuvant TEMozolomide followed by chemoradiotherapy versus upfront chemoradiotherapy for glioblastoma multiforme (NEOTEM) trial: Interim results.Neurooncol Adv. 2024 Nov 14;6(1):vdae195. doi: 10.1093/noajnl/vdae195. eCollection 2024 Jan-Dec. Neurooncol Adv. 2024. PMID: 39664679 Free PMC article.
-
The role of radiotherapy in the management of metastatic rectal cancer: A narrative review on the opportunities for non-operative management and organ preservation.Clin Transl Radiat Oncol. 2025 May 4;53:100976. doi: 10.1016/j.ctro.2025.100976. eCollection 2025 Jul. Clin Transl Radiat Oncol. 2025. PMID: 40469947 Free PMC article. Review.
-
Short-course versus long-course neoadjuvant chemoradiotherapy in patients with rectal cancer: long-term results of a randomized controlled trial.Int J Colorectal Dis. 2025 May 14;40(1):118. doi: 10.1007/s00384-025-04901-1. Int J Colorectal Dis. 2025. PMID: 40369294 Free PMC article. Clinical Trial.
References
-
- Petrelli F., Trevisan F., Cabiddu M., et al., “Total Neoadjuvant Therapy in Rectal Cancer: A Systematic Review and Meta‐Analysis of Treatment Outcomes,” Annals of Surgery 271, no. 3 (2020): 440–448. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
