

Assessing tumor microstructure with time-dependent diffusion imaging: Considerations and feasibility on clinical MRI and MRI-Linac
- PMID: 39387639
- PMCID: PMC11700005
- DOI: 10.1002/mp.17453
Assessing tumor microstructure with time-dependent diffusion imaging: Considerations and feasibility on clinical MRI and MRI-Linac
Abstract
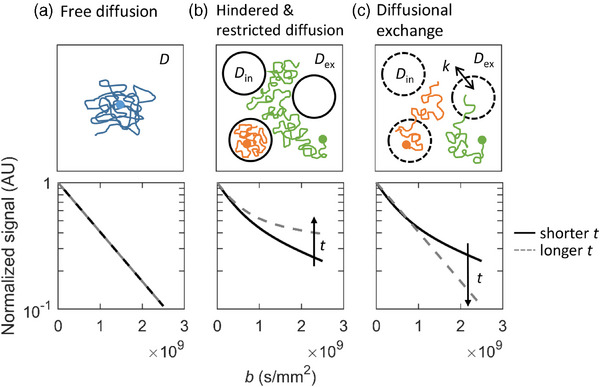
Background: Quantitative imaging biomarkers (QIBs) can characterize tumor heterogeneity and provide information for biological guidance in radiotherapy (RT). Time-dependent diffusion MRI (TDD-MRI) derived parameters are promising QIBs, as they describe tissue microstructure with more specificity than traditional diffusion-weighted MRI (DW-MRI). Specifically, TDD-MRI can provide information about both restricted diffusion and diffusional exchange, which are the two time-dependent effects affecting diffusion in tissue, and relevant in tumors. However, exhaustive modeling of both effects can require long acquisitions and complex model fitting. Furthermore, several introduced TDD-MRI measurements can require high gradient strengths and/or complex gradient waveforms that are possibly not available in RT settings.
Purpose: In this study, we investigated the feasibility of a simple analysis framework for the detection of restricted diffusion and diffusional exchange effects in the TDD-MRI signal. To promote the clinical applicability, we use standard gradient waveforms on a conventional 1.5 T MRI system with moderate gradient strength (Gmax = 45 mT/m), and on a hybrid 1.5 T MRI-Linac system with low gradient strength (Gmax = 15 mT/m).
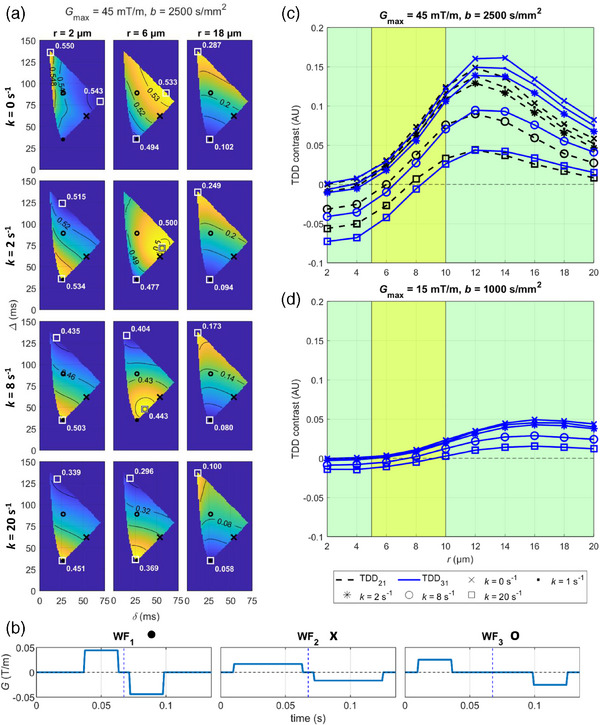
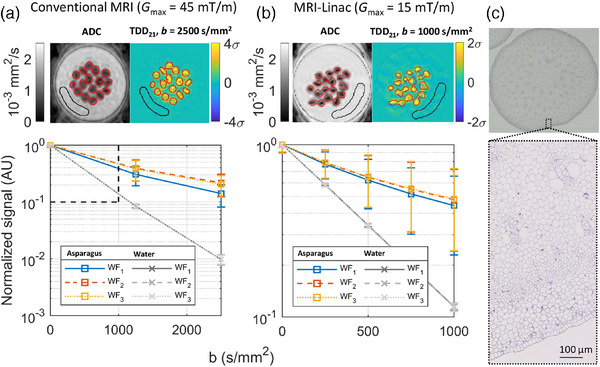
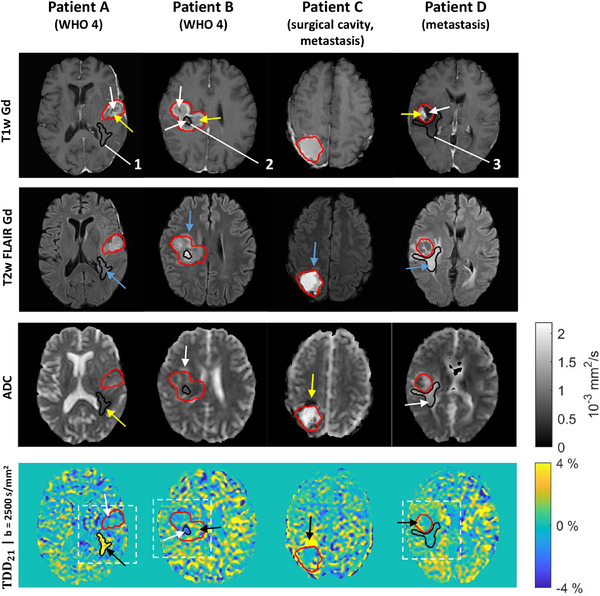
Methods: Restricted diffusion and diffusional exchange were simulated in geometries mimicking tumor microstructure to investigate the DW-MRI signal behavior and to determine optimal experimental parameters. TDD-MRI was implemented using pulsed field gradient spin echo with the optimized parameters on a conventional MRI system and a MRI-Linac. Experiments in green asparagus and 10 patients with brain lesions were performed to evaluate the time-dependent diffusion (TDD) contrast in the source DW-images.
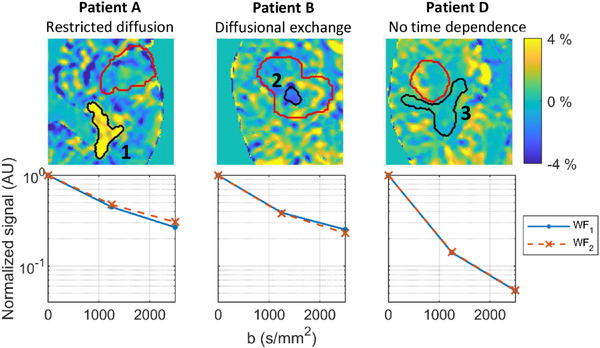
Results: Simulations demonstrated how the TDD contrast was able to differentiate only dominating diffusional exchange in smaller cells from dominating restricted diffusion in larger cells. The maximal TDD contrast in simulations with typical cancer cell sizes and in asparagus measurements exceeded 5% on the conventional MRI but remained below 5% on the MRI-Linac. In particular, the simulated TDD contrast in typical cancer cell sizes (r = 5-10 µm) remained below or around 2% with the MRI-Linac gradient strength. In patients measured with the conventional MRI, we found sub-regions reflecting either dominating restricted diffusion or dominating diffusional exchange in and around brain lesions compared to the noisy appearing white matter.
Conclusions: On the conventional MRI system, the TDD contrast maps showed consistent tumor sub-regions indicating different dominating TDD effects, potentially providing information on the spatial tumor heterogeneity. On the MRI-Linac, the available TDD contrast measured in asparagus showed the same trends as with the conventional MRI but remained close to typical measurement noise levels when simulated in common cancer cell sizes. On conventional MRI systems with moderate gradient strengths, the TDD contrast could potentially be used as a tool to identify which time-dependent effects to include when choosing a biophysical model for more specific tumor characterization.
Keywords: biologically guided radiotherapy; biophysical modeling; diffusion MRI; imaging biomarkers; time‐dependent diffusion.
© 2024 The Author(s). Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
H.L. is an inventor and has an interest in patents owned by RWI AB, Lund, Sweden, related to DW‐MRI methodologies not applied in this work. All other authors declare no conflicts of interest.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
