

Socioeconomic disparities and cardio-cerebrovascular diseases: A nationwide cross-sectional study
- PMID: 39388680
- PMCID: PMC11466497
- DOI: 10.7189/jogh.14.04210
Socioeconomic disparities and cardio-cerebrovascular diseases: A nationwide cross-sectional study
Abstract
Background: Although socioeconomic status (SES) is considered a risk factor for cardio-cerebrovascular diseases (CCVDs), few studies have examined this association. In this cross-sectional study, we aimed to assess the prevalence and trends of CCVDs across different SES groups over a 12-year period in a representative Korean population.
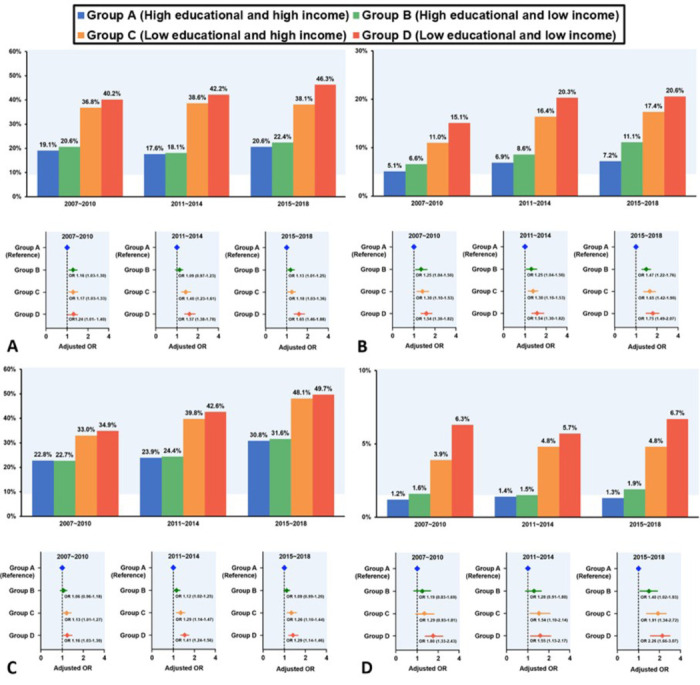
Methods: We analysed 47 745 economically active adults aged ≥30 and <65 years from 97 622 patients in the Korean National Health and Nutrition Examination Survey (2007-18), where a new independent sample of the population was examined each year. We categorised the participants into four groups based on education level and income. The prevalence of hypertension, diabetes mellitus, dyslipidaemia, and CCVD, including angina, myocardial infarction, and stroke, was analysed at four-year intervals.
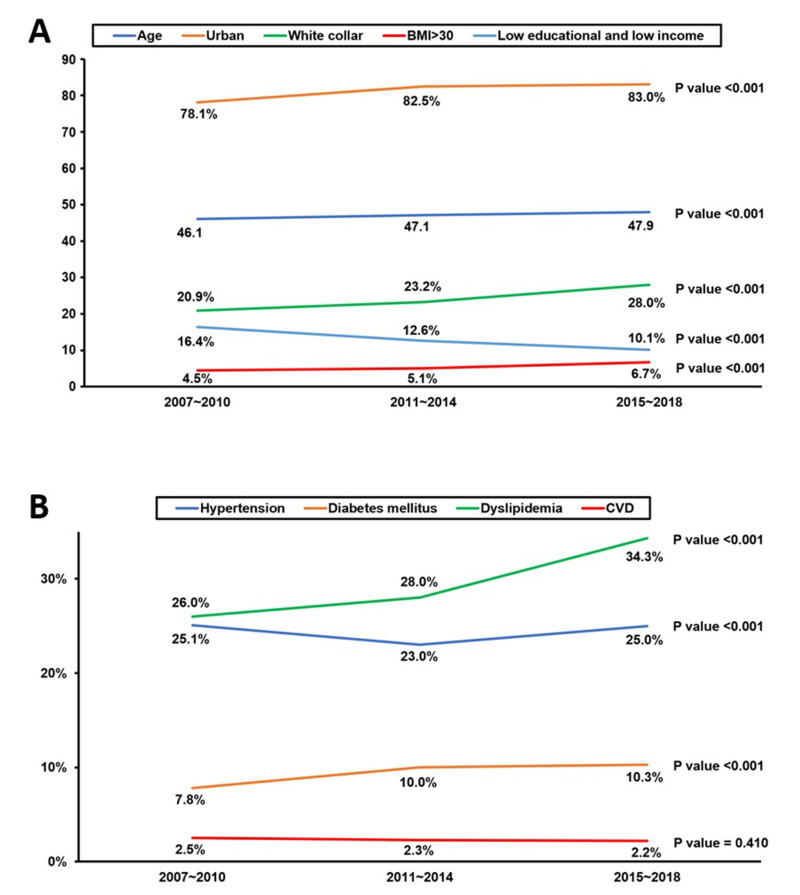
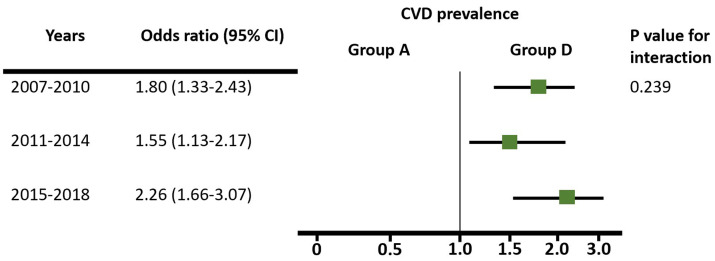
Results: Average age, urban residence, white-collar occupation, and body mass index >30 increased, whereas CCVD prevalence did not change significantly (P = 0.410) over the study period. Low education (odds ratio (OR) = 1.24; 95% confidence interval (CI) = 1.04-1.47, P < 0.001) and low income (OR = 1.14; 95% CI = 1.02-1.28, P = 0.017) were significant determinants of CCVD in addition to existing traditional risk factors. CCVD prevalence was significantly higher in both the low-education and low-income groups compared to the high-education and high-income groups every four years, with no significant change in this gap over the study period (P = 0.239).
Conclusions: Despite the increase in the elderly population and the prevalence of obesity, the incidence of CCVDs in Korea has remained unchanged. Individuals with low education or low income had a significantly higher prevalence of CCVD, with the lowest SES group, defined by both low education and low income, consistently having the highest prevalence of CCVDs.
Copyright © 2024 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interest.
Figures
References
-
- Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395:795–808. 10.1016/S0140-6736(19)32008-2 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
