

Infant-derived human nasal organoids exhibit relatively increased susceptibility, epithelial responses, and cytotoxicity during RSV infection
- PMID: 39389204
- PMCID: PMC12067953
- DOI: 10.1016/j.jinf.2024.106305
Infant-derived human nasal organoids exhibit relatively increased susceptibility, epithelial responses, and cytotoxicity during RSV infection
Abstract
Background: Respiratory syncytial virus (RSV) causes significant morbidity and mortality, especially in young children. Why RSV infection in children is more severe compared to healthy adults is not fully understood.
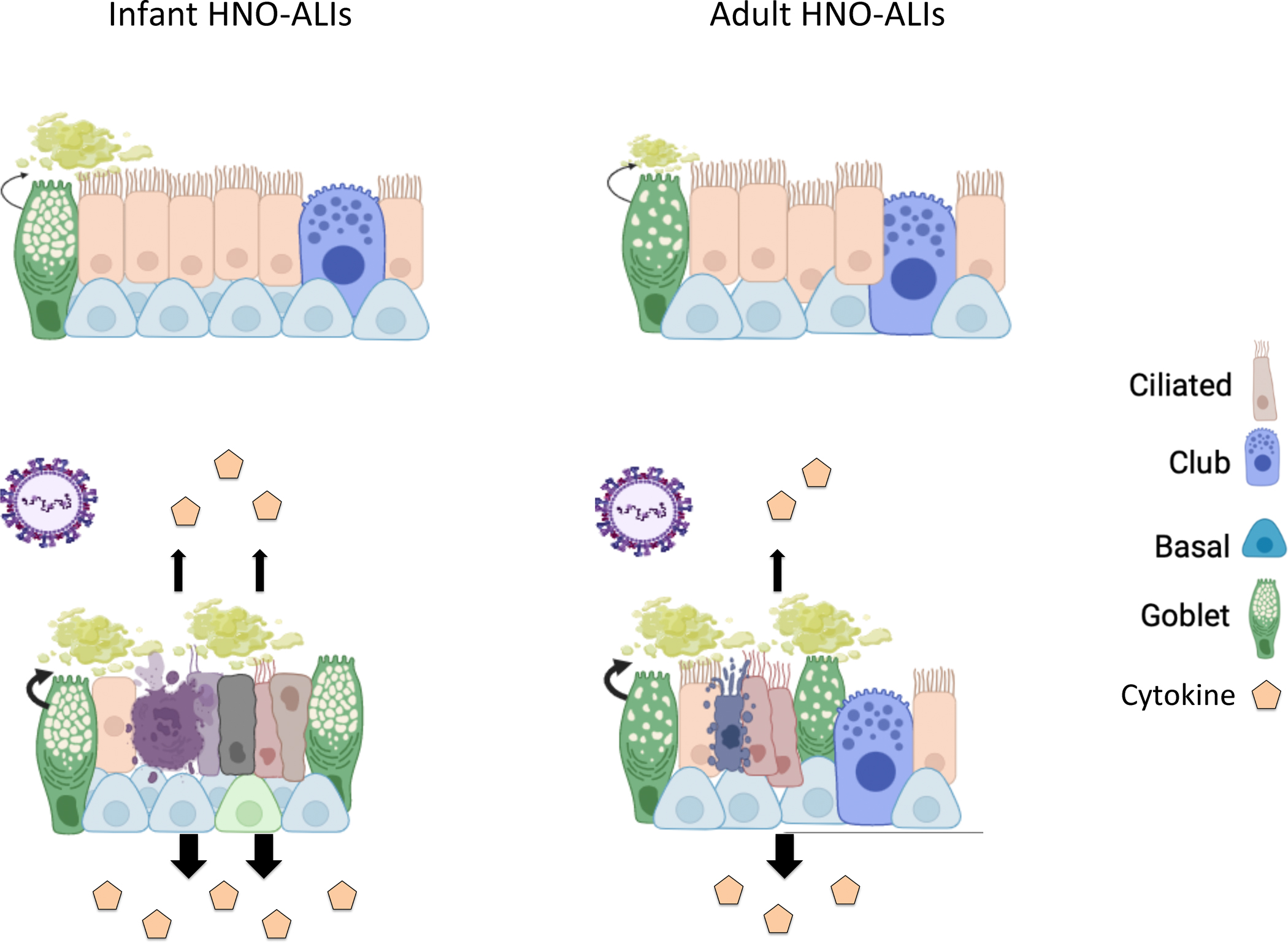
Methods: We used ex-vivo human nasal organoid platforms from infants and adults to investigate the underlying mechanism of this disease disparity at the initial site of RSV replication, the nasal epithelium.
Results: Infant-derived human nasal organoid-air liquid interface (HNO-ALIs) lines were more susceptible to early RSV replication. Moreover, infant-derived HNO-ALIs elicited a statistically significant greater overall cytokine response, enhanced mucous production, and greater cellular damage compared to their adult counterparts. Furthermore, the adult cytokine response was associated with a superior regulatory cytokine response, which could explain less cellular damage than in infant lines.
Conclusions: Our data highlights substantial differences in how infant and adult upper respiratory tract epithelium responds to RSV infection at the cellular level. These differences in epithelial cellular response can lead to impaired mucociliary clearance, a more dysregulated innate immune response predisposing infants to more severe RSV infection compared to adults.
Keywords: Adult; Infant; Infection; Innate immune responses; Nasal organoids; RSV; Replication.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare no conflicts of interest.
Figures







Update of
-
Pediatric human nose organoids demonstrate greater susceptibility, epithelial responses, and cytotoxicity than adults during RSV infection.bioRxiv [Preprint]. 2024 Feb 1:2024.02.01.578466. doi: 10.1101/2024.02.01.578466. bioRxiv. 2024. Update in: J Infect. 2024 Dec;89(6):106305. doi: 10.1016/j.jinf.2024.106305. PMID: 38352333 Free PMC article. Updated. Preprint.
References
-
- Meissner HC. Viral Bronchiolitis in Children. N Engl J Med. 2016;374(1):62–72. - PubMed
-
- Smith DK, Seales S, Budzik C. Respiratory Syncytial Virus Bronchiolitis in Children. Am Fam Physician. 2017;95(2):94–99. - PubMed
-
- Glezen WP, et al. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child. 1986;140(6):543–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
