

Heart failure diagnostic accuracy, intraoperative fluid management, and postoperative acute kidney injury: a single-centre prospective observational study
- PMID: 39389834
- PMCID: PMC11832916
- DOI: 10.1016/j.bja.2024.08.020
Heart failure diagnostic accuracy, intraoperative fluid management, and postoperative acute kidney injury: a single-centre prospective observational study
Erratum in
-
Corrigendum to 'Heart failure diagnostic accuracy, intraoperative fluid management, and postoperative acute kidney injury: a single-centre prospective observational study' [Br J Anaesth 2025; 134: 32-44].Br J Anaesth. 2025 Sep;135(3):828. doi: 10.1016/j.bja.2025.06.012. Epub 2025 Jul 11. Br J Anaesth. 2025. PMID: 40651875 Free PMC article. No abstract available.
Abstract
Background: The accurate diagnosis of heart failure (HF) before major noncardiac surgery is frequently challenging. The impact of diagnostic accuracy for HF on intraoperative practice patterns and clinical outcomes remains unknown.
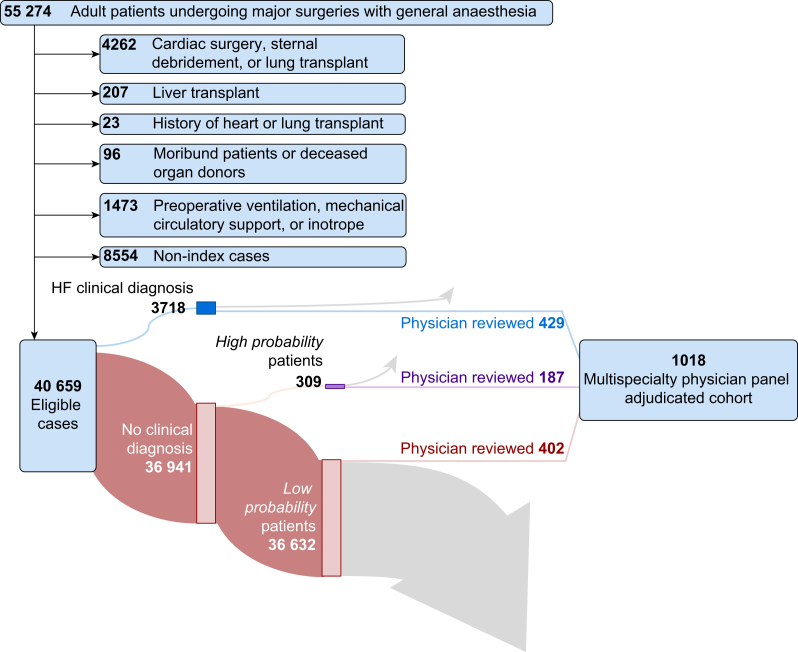
Methods: We performed an observational study of adult patients undergoing major noncardiac surgery at an academic hospital from 2015 to 2019. A preoperative clinical diagnosis of HF was defined by keywords in the preoperative assessment or a diagnosis code. Medical records of patients with and without HF clinical diagnoses were reviewed by a multispecialty panel of physician experts to develop an adjudicated HF reference standard. The exposure of interest was an adjudicated diagnosis of heart failure. The primary outcome was volume of intraoperative fluid administered. The secondary outcome was postoperative acute kidney injury (AKI).
Results: From 40 659 surgeries, a stratified subsample of 1018 patients were reviewed by a physician panel. Among patients with adjudicated diagnoses of HF, those without a clinical diagnosis (false negatives) more commonly had preserved left ventricular ejection fractions and fewer comorbidities. Compared with false negatives, an accurate diagnosis of HF (true positives) was associated with 470 ml (95% confidence interval: 120-830; P=0.009) lower intraoperative fluid administration and lower risk of AKI (adjusted odds ratio:0.39, 95% confidence interval 0.18-0.89). For patients without adjudicated diagnoses of HF, non-HF was not associated with differences in either fluids administered or AKI.
Conclusions: An accurate preoperative diagnosis of heart failure before noncardiac surgery is associated with reduced intraoperative fluid administration and less acute kidney injury. Targeted efforts to improve preoperative diagnostic accuracy for heart failure may improve perioperative outcomes.
Keywords: acute kidney injury; diagnostic accuracy; electronic health record; heart failure; intraoperative fluid management; noncardiac surgery; preoperative evaluation.
Published by Elsevier Ltd.
Figures

References
-
- Duceppe E., Patel A., Chan M.T.V., et al. Preoperative N-terminal pro-B-type natriuretic peptide and cardiovascular events after noncardiac surgery: a cohort study. Ann Intern Med. 2020;172:96–104. - PubMed
-
- Smit-Fun V., Buhre W.F. The patient with chronic heart failure undergoing surgery. Curr Opin Anaesthesiol. 2016;29:391–396. - PubMed
-
- Xu-Cai Y.O., Brotman D.J., Phillips C.O., et al. Outcomes of patients with stable heart failure undergoing elective noncardiac surgery. Mayo Clin Proc. 2008;83:280–288. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
