

Predicting future hospital antimicrobial resistance prevalence using machine learning
- PMID: 39390045
- PMCID: PMC11467333
- DOI: 10.1038/s43856-024-00606-8
Predicting future hospital antimicrobial resistance prevalence using machine learning
Abstract
Background: Predicting antimicrobial resistance (AMR), a top global health threat, nationwide at an aggregate hospital level could help target interventions. Using machine learning, we exploit historical AMR and antimicrobial usage to predict future AMR.
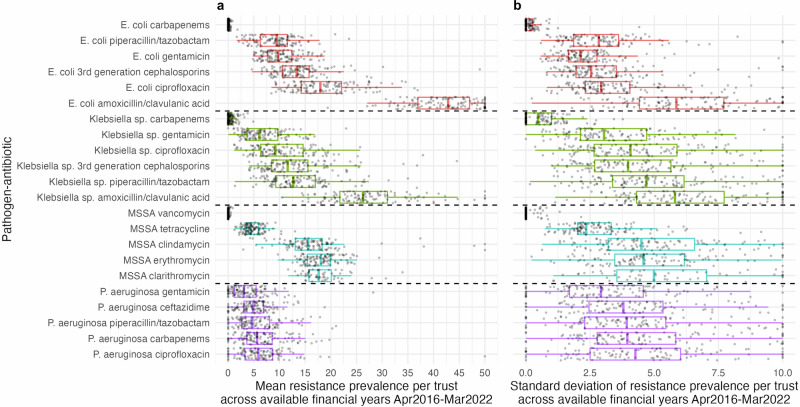
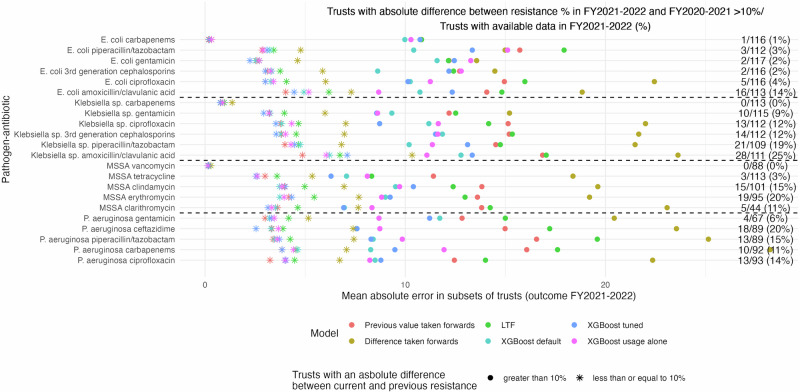
Methods: Antimicrobial use and AMR prevalence in bloodstream infections in hospitals in England were obtained per hospital group (Trust) and financial year (FY, April-March) for 22 pathogen-antibiotic combinations (FY2016-2017 to FY2021-2022). Extreme Gradient Boosting (XGBoost) model predictions were compared to the previous value taken forwards, the difference between the previous two years taken forwards and linear trend forecasting (LTF). XGBoost feature importances were calculated to aid interpretability.
Results: Here we show that XGBoost models achieve the best predictive performance. Relatively limited year-to-year variability in AMR prevalence within Trust-pathogen-antibiotic combinations means previous value taken forwards also achieves a low mean absolute error (MAE), similar to or slightly higher than XGBoost. Using the difference between the previous two years taken forward or LTF performs consistently worse. XGBoost considerably outperforms all other methods in Trusts with a larger change in AMR prevalence from FY2020-2021 (last training year) to FY2021-2022 (held-out test set). Feature importance values indicate that besides historical resistance to the same pathogen-antibiotic combination as the outcome, complex relationships between resistance in different pathogens to the same antibiotic/antibiotic class and usage are exploited for predictions. These are generally among the top ten features ranked according to their mean absolute SHAP values.
Conclusions: Year-to-year resistance has generally changed little within Trust-pathogen-antibiotic combinations. In those with larger changes, XGBoost models can improve predictions, enabling informed decisions, efficient resource allocation, and targeted interventions.
Plain language summary
Antibiotics play an important role in treating serious bacterial infections. However, with the increased usage of antibiotics, they are becoming less effective. In our study, we use machine learning to learn from past antibiotic resistance and usage in order to predict what resistance will look like in the future. Different hospitals across England have very different resistance levels, however, within each hospital, these levels remain stable over time. When larger changes in resistance occurred over time in individual hospitals, our methods were able to predict these. Understanding how much resistance there is in hospital populations, and what may occur in the future can help determine where resources and interventions should be directed.
© 2024. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: D.W.E. declares lecture fees from Gilead, outside the submitted work. Authors K.-D.V., E.P., K.B.P., S.H., R.L.G., K H., D.C., R.H., B.M.-P., A.S.W., D.C. declare no competing interests.
Figures


References
-
- World Health Organization. Antimicrobial Resistance (WHO, accessed 10 August 2023); https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance.
-
- Baquero, F. & Negri, M. Antibiotic-selective environments. Clin. Infect. Dis.27, 5–11 (1998). - PubMed
-
- Goossens, H., Ferech, M., Vander Stichele, R. & Elseviers, M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet365, 579–587 (2005). - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
