

Discovery of prognostic lncRNAs in colorectal cancer using spatial transcriptomics
- PMID: 39390212
- PMCID: PMC11467462
- DOI: 10.1038/s41698-024-00728-1
Discovery of prognostic lncRNAs in colorectal cancer using spatial transcriptomics
Abstract
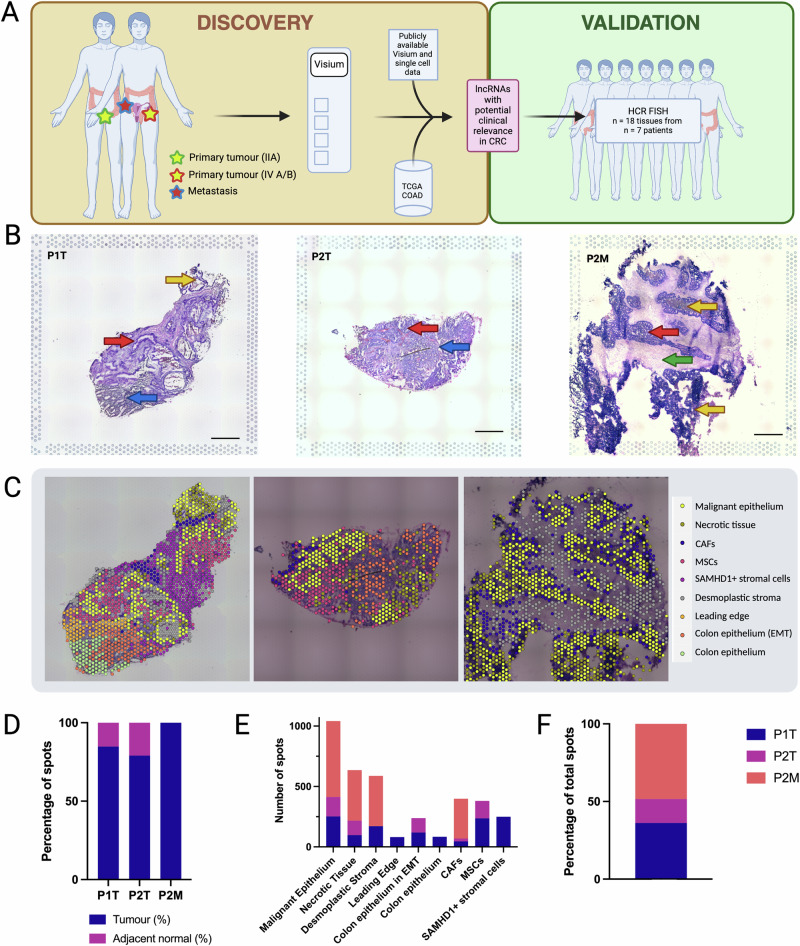
Colorectal cancer (CRC) exhibits significant genetic and epigenetic diversity, evolving into sub-clonal populations with varied metastatic potentials and treatment responses. Predicting metastatic disease in CRC patients remains challenging, underscoring the need for reliable biomarkers. While most research on therapeutic targets and biomarkers has focused on proteins, non-coding RNAs such as long non-coding RNAs (lncRNAs) comprise most of the transcriptome and demonstrate superior tissue- and cancer-specific expression. We utilised spatial transcriptomics to investigate lncRNAs in CRC tumours, offering more precise cell-type-specific expression data compared to bulk RNA sequencing. Our analysis identified 301 lncRNAs linked to malignant CRC regions, which we validated with public data. Further validation using RNA-FISH revealed three lncRNAs (LINC01978, PLAC4, and LINC01303) that are detectable in stage II tumours but not in normal epithelium and are upregulated in metastatic tissues. These lncRNAs hold potential as biomarkers for early risk assessment of metastatic disease.
© 2024. The Author(s).
Conflict of interest statement
Author S.D.D. is a cofounder and consultant to, and holds shares in, Amaroq Therapeutics and RNAfold.AI, but declares no competing interests. The remaining authors declare no competing interests.
Figures



References
-
- Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin.10.3322/caac.21660 (2021). - PubMed
-
- Ferlay, J. et al. Global Cancer Observatory: Cancer Today (version 1.1). (International Agency for Research on Cancer, Lyon, France, 2024). https://gco.iarc.who.int/today [cited 19 Mar 2024].
-
- Siegel, R. L., Miller, K. D., Wagle, N. S. & Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin.73, 17–48 (2023). - PubMed
-
- Fearon, E. R. Molecular genetics of colorectal cancer. Annu Rev. Pathol.6, 479–507 (2011). - PubMed
LinkOut - more resources
Full Text Sources
