

Insight of autonomic dysfunction in CLN3 disease: a study on episodes resembling paroxysmal sympathetic hyperactivity (PSH)
- PMID: 39390491
- PMCID: PMC11465670
- DOI: 10.1186/s13023-024-03336-1
Insight of autonomic dysfunction in CLN3 disease: a study on episodes resembling paroxysmal sympathetic hyperactivity (PSH)
Abstract
Background: Recurrent non-epileptic episodes resembling paroxysmal sympathetic hyperactivity (PSH) have been observed in adolescents with Juvenile Ceroid Lipofuscinosis (CLN3-disease) and a possible association to an autonomic dysfunction has been suggested. The objective of the present study was to investigate the dynamics of the autonomic activity up to, during, and in the time after individual attacks. We include all seven suitable CLN3 patients in Denmark ≥ 15 years of age. HRV parameters were assessed from continuous heart rate monitoring during seven consecutive days and a particular focus of HRV parameters was obtained in close temporal context to clinically recurrent PSH-like episodes. In addition, the likelihood of PSH was assessed by caregiver's description and by video documentation.
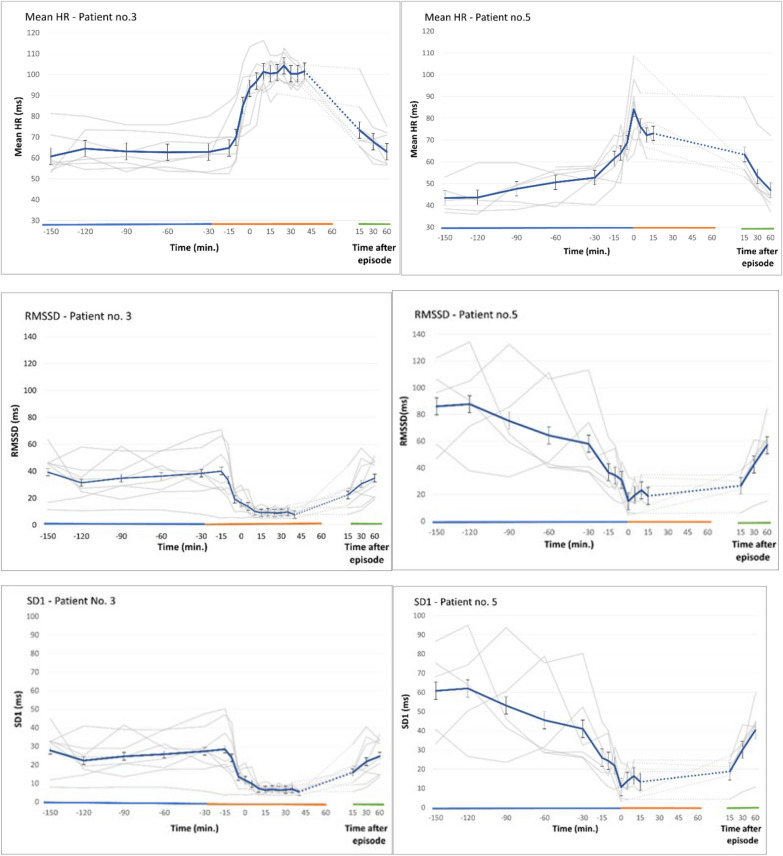
Results: Respectively eight and five episodes were recorded in two patients (18 and 20 years of age). The episodes were all safely superior to the cut off values of the clinical assessment score to be considered PSH-like episodes. During all 13 episodes, HRV revealed a statistically significant decrease in root mean square of successive differences (RMSSD) and standard deviation of the Poincaré-Plot interval (SD1) in the minutes prior to the clinical onset of the episodes, both indicating a sudden decrease in parasympathetic activity in advance of the onset. The reduced activity remained low during the episodes, and 15-30 min following the attack cessation, the parasympathetic activity had returned to pre-attacks levels. The sympathetic HRV parameters were unchanged resulting in a sympathetic overactivity during the episodes. In a third participant (32 years of age), in whom severity of PSH-like episodes had been gradually reduced during the last years, five episodes were registered. A similar temporally related reduction of the parasympathetic activity was found, but because the sympathetic activity decreased as well, no sympathetic dominance developed, which most reasonable is the reason to the clinically reduced expression of the episodes.
Conclusion: The documented transient withdrawal of parasympathetic activity leading to a paroxysmal unbalanced sympathetic hyperactivity most probably accounts for the PSH-like episodes occurring in post-adolescent CLN3 patients. The findings shed new light on both aetiology and possible preventative and therapeutic measures.
Keywords: Autonomic dysfunction; CLN3; JNCL; Neuronal ceroid lipofuscinosis; PSH.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Jalanko A, Braulke T. Neuronal ceroid lipofuscinoses. Biochim Biophys Acta. 2009;1793(4):697–709. - PubMed
-
- Ostergaard JR, Rasmussen TB, Mølgaard H. Cardiac involvement in juvenile neuronal ceroid lipofuscinosis (Batten disease). Neurology. 2011;76(14):1245–51. - PubMed
-
- Sørensen JB, Parnas J. A clinical study of 44 patients with juvenile amaurotic family idiocy. Acta Psychiatr Scand. 1979;59(5):449–61. - PubMed
-
- Hofman IL. Observations in institutionalized neuronal ceroid-lipofuscinosis patients with special reference to involuntary movements. J Inherit Metab Dis. 1993;16(2):249–51. - PubMed
-
- Baguley IJ. The excitatory:inhibitory ratio model (EIR model): An integrative explanation of acute autonomic overactivity syndromes. Med Hypotheses. 2008;70(1):26–35. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
