

Advanced MRI Measures of Myelin and Axon Volume Identify Repair in Multiple Sclerosis
- PMID: 39390658
- PMCID: PMC11683175
- DOI: 10.1002/ana.27102
Advanced MRI Measures of Myelin and Axon Volume Identify Repair in Multiple Sclerosis
Abstract
Objective: Pathological studies suggest that multiple sclerosis (MS) lesions endure multiple waves of damage and repair; however, the dynamics and characteristics of these processes are poorly understood in patients living with MS.
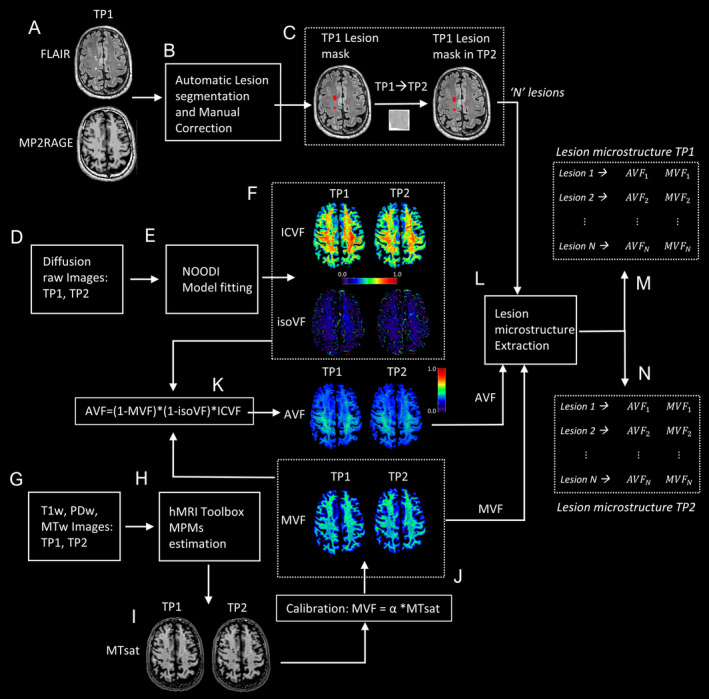
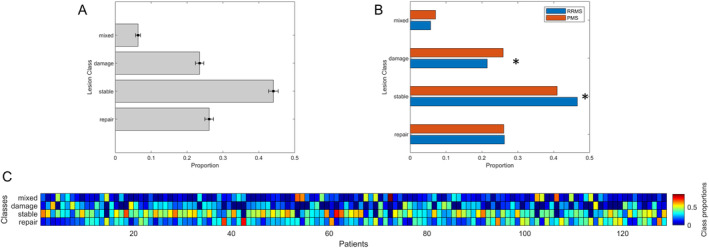
Methods: We studied 128 MS patients (75 relapsing-remitting, 53 progressive) and 72 healthy controls who underwent advanced magnetic resonance imaging and clinical examination at baseline and 2 years later. Magnetization transfer saturation and multi-shell diffusion imaging were used to quantify longitudinal changes in myelin and axon volumes within MS lesions. Lesions were grouped into 4 classes (repair, damage, mixed repair damage, and stable). The frequency of each class was correlated to clinical measures, demographic characteristics, and levels of serum neurofilament light chain (sNfL).
Results: Stable lesions were the most frequent (n = 2,276; 44%), followed by lesions with patterns of "repair" (n = 1,352; 26.2%) and damage (n = 1,214; 23.5%). The frequency of "repair" lesion was negatively associated with disability (β = -0.04; p < 0.001) and sNfL (β = -0.16; p < 0.001) at follow-up. The frequency of the "damage" class was higher in progressive than relapsing-remitting patients (p < 0.05) and was related to disability (baseline: β = -0.078; follow-up: β = -0.076; p < 0.001) and age (baseline: β = -0.078; p < 0.001). Stable lesions were more frequent in relapsing-remitting than in progressive patients (p < 0.05), and in younger patients versus older (β = -0.07; p < 0.001) at baseline. Further, "mixed" lesions were most frequent in older patients (β = 0.004; p < 0.001) at baseline.
Interpretation: These findings show that repair and damage processes within MS lesions occur across the entire disease spectrum and that their frequency correlates with patients disability, age, disease duration, and extent of neuroaxonal damage. ANN NEUROL 2024.
© 2024 The Author(s). Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
J.K. has received grants and consulting fees and has been part of the data safety monitoring board and advisor board for different companies (Biogen, Merck, Novartis, Roche). The remaining authors have no relevant conflicts of interest to declare. A.C. has received payment from lectures, presentations and as speaker from Novartis. L.C. has received grant contracts, consulting fees, payment as speaker, participate on data safety monitoring board and advisor board and as leadership for different companies such as Innosuisse, Novartis, Roche, Bayer, Biogen, Janssen, Sanofi, and Bristol Myers Squibb.
Figures




References
Grants and funding
LinkOut - more resources
Full Text Sources
