

Evaluation of immune checkpoint inhibitors for colorectal cancer: A network meta‑analysis
- PMID: 39390977
- PMCID: PMC11465421
- DOI: 10.3892/ol.2024.14702
Evaluation of immune checkpoint inhibitors for colorectal cancer: A network meta‑analysis
Abstract
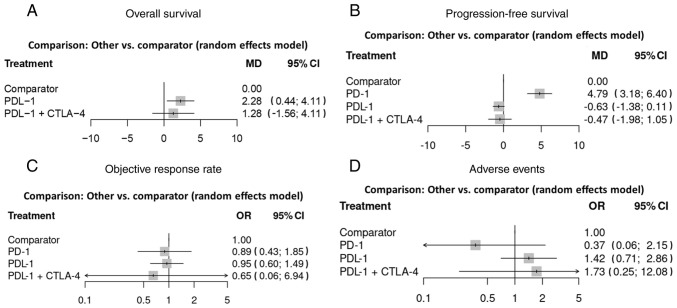
Colorectal cancer (CRC) is challenging to treat due to its high metastatic rate. Recent strategies have focused on combining immune checkpoint inhibitors (ICIs) with other treatments. The aim of the present study was to conduct a network meta-analysis of randomized controlled trials (RCTs) to assess the efficacy and adverse effects of different ICI treatments for CRC. A literature search for RCTs was conducted using PubMed, the Cochrane Library, Embase, ClinicalTrials.gov and Web of Science databases, covering the period from the inception of each database until April 2024. A total of 12 RCTs involving 2,050 participants were selected for inclusion in the analysis. The network meta-analysis employed the MetaInsight tool to assess multiple endpoints. The criteria for study selection were based on the Population, Intervention, Comparison, Outcome and Studies framework as follows: i) Population, patients with CRC; ii) intervention, studies using ICI to treat CRC; iii) comparison, active comparators, including placebo; iv) outcome, overall survival, progression-free survival, objective response rate and adverse events; and v) study design, RCTs. The results of the analysis revealed that programmed cell death-ligand 1 (PD-L1) inhibitors significantly improved overall survival time [mean difference (MD), 2.28 months; 95% confidence interval (CI), 0.44 to 4.11], while programmed cell death protein 1 (PD-1) inhibitors exhibited a superior progression-free survival time (MD, 4.79 months; 95% CI, 3.18 to 6.40) compared with active comparators. However, none of the ICI treatments had significant differences in odds ratios for the objective response rate and adverse events compared with active comparators. These findings indicate that treatment with PD-L1 and PD-1 inhibitors improved the overall survival time and delayed disease progression in patients with CRC. These findings offer valuable insights for future research aimed at improving CRC patient outcomes.
Keywords: colon; immunotherapy; neoplasm; rectum; survival.
Copyright: © Tzang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





Similar articles
-
Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2020 Dec 14;12(12):CD013257. doi: 10.1002/14651858.CD013257.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 30;4:CD013257. doi: 10.1002/14651858.CD013257.pub3. PMID: 33316104 Free PMC article. Updated.
-
Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2021 Apr 30;4(4):CD013257. doi: 10.1002/14651858.CD013257.pub3. Cochrane Database Syst Rev. 2021. PMID: 33930176 Free PMC article.
-
Immune checkpoint inhibitors for patients with microsatellite instability-high colorectal cancer: protocol of a pooled analysis of clinical trials.Front Oncol. 2024 Jan 3;13:1331937. doi: 10.3389/fonc.2023.1331937. eCollection 2023. Front Oncol. 2024. PMID: 38234398 Free PMC article.
-
Efficacy and safety of immune checkpoint inhibitors in colorectal cancer: a systematic review and meta-analysis.Int J Colorectal Dis. 2022 Jan;37(1):251-258. doi: 10.1007/s00384-021-04028-z. Epub 2021 Oct 29. Int J Colorectal Dis. 2022. PMID: 34716473 Free PMC article.
-
Efficacy and predictive factors of immune checkpoint inhibitors in metastatic breast cancer: a systematic review and meta-analysis.Ther Adv Med Oncol. 2020 Aug 17;12:1758835920940928. doi: 10.1177/1758835920940928. eCollection 2020. Ther Adv Med Oncol. 2020. PMID: 32874208 Free PMC article.
Cited by
-
Prognostic impact of syndecan-1 expression and serum concentration in colorectal cancer.Oncol Lett. 2025 Jun 19;30(2):402. doi: 10.3892/ol.2025.15148. eCollection 2025 Aug. Oncol Lett. 2025. PMID: 40606308 Free PMC article.
References
-
- Hossain MS, Karuniawati H, Jairoun AA, Urbi Z, Ooi J, John A, Lim YC, Kibria KMK, Mohiuddin AKM, Ming LC, et al. Colorectal cancer: A review of carcinogenesis, global epidemiology, current challenges, risk factors, preventive and treatment strategies. Cancers (Basel) 2022;14:1732. doi: 10.3390/cancers14071732. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous