

Feasibility of opioid-free anesthesia in laparoscopic radical prostatectomy: A retrospective, quasi-experimental study
- PMID: 39391640
- PMCID: PMC11463948
- DOI: 10.4103/joacp.joacp_375_23
Feasibility of opioid-free anesthesia in laparoscopic radical prostatectomy: A retrospective, quasi-experimental study
Abstract
Background and aims: Opioid-free anesthesia (OFA) provides adequate analgesia minimizing opioids. OFA has not been evaluated in laparoscopic radical prostatectomy (LRP). Our aim was to evaluate OFA feasibility and its effectiveness in LRP.
Material and methods: A quasi-experimental retrospective study of 55 adult patients undergoing LRP was performed from September 2020 until December 20223. Predefined protocols for either opioid-based anesthesia (OBA; with continuous remifentanil infusion) or OFA (continuous lidocaine, dexmedetomidine, and ketamine infusion) were followed. In both groups, wound infiltration was performed before skin incision. Primary outcome was postoperative pain management (numerical rating scale [NRS]) in the first 24 postoperative hours. Secondary outcomes were opioid consumption, start to sitting and ambulation, postoperative complications, and length of hospital stay.
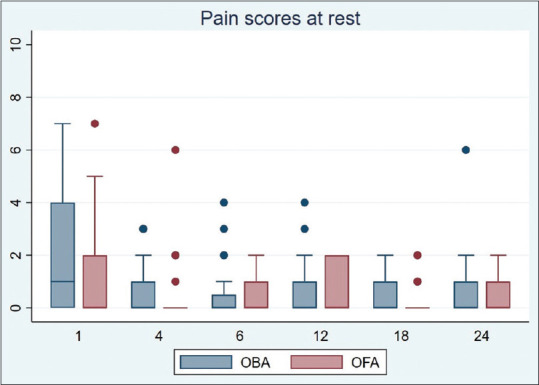
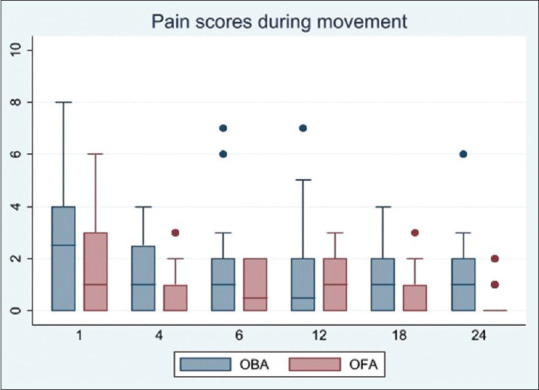
Results: OFA protocol patients had better median pain scores during movement at 1, 18 and 24 h, that is, 1 (interquartile range [IQR] 0-3) versus 2.5 (IQR 0-4), P = 0.047; 0 (IQR 0-1) versus 1 (IQR 0-2), P = 0.017; and 0 (IQR 0-0.25) versus 1 (IQR 0-2), P = 0.013, respectively. At 6 and 12 h, there were no statistically significant differences, that is, 0.5 (IQR 0-2) versus 1 (IQR 0-2), P = 0.908 and 1 (IQR 0-2) versus 0.5 (IQR 0-2), P = 0.929, respectively. Lower morphine requirements were recorded in the first 18 and 24 postoperative hours, that is, 0 (IQR 0-0) versus 1 (IQR 0-2.75) mg, P = 0.028 and 0 (IQR 0-2) versus 1.5 (IQR 0-3) mg, P = 0.012, respectively. Start to sitting and ambulation occurred earlier in the OFA group (P = 0.030 and P = 0.002, respectively). Linear regression showed that ambulation was independently associated with the analgesic technique (P = 0.034). Only one patient had postoperative nausea and vomiting (PONV) and belonged to the OBA group. There was no difference in total complications or the length of stay.
Conclusion: In this study, OFA strategy was found to be safe, feasible, and provided adequate analgesia, minimizing the use of postoperative opioids, and was independently associated with earlier ambulation.
Keywords: Analgesia; dexmedetomidine; enhanced recovery after surgery; ketamine; laparoscopic prostatectomy; lidocaine; morphine; opioid-free; postoperative Pain; remifentanil.
Copyright: © 2024 Journal of Anaesthesiology Clinical Pharmacology.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential Elements of multimodal analgesia in enhanced recovery after surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35:e115–43. - PubMed
-
- Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesia pain management with nonopioid analgesics and techniques: A review. JAMA Surg. 2017;152:691–7. - PubMed
-
- Brown RE, Sloan PA. The opioid crisis in the United States: Chronic pain physicians are the answer, not the cause. Anesth Analg. 2017;125:1432–4. - PubMed
-
- Theisen KM, Myrga JM, Hale N, Cochran G, Sewall C, Macleod LC, et al. Excessive opioid prescribing after major urologic procedures. Urology. 2019;123:101–7. - PubMed
-
- Tsui C, Klein R, Garabrant M. Minimally invasive surgery: National trends in adoption and future directions for hospital strategy. Surg Endosc. 2013;27:2253–7. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous