

SDMA as a marker and mediator in cerebrovascular disease
- PMID: 39391895
- PMCID: PMC11479986
- DOI: 10.1042/CS20241021
SDMA as a marker and mediator in cerebrovascular disease
Abstract
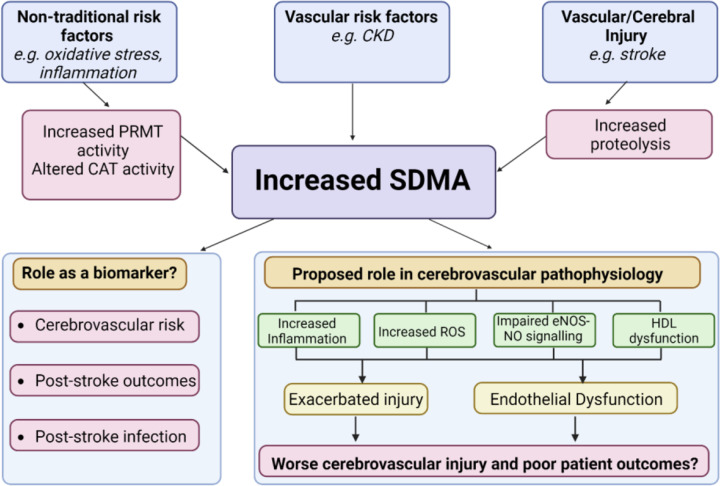
Symmetric dimethylarginine (SDMA) is a methylated derivative of arginine, generated by all cells as a by-product of cellular metabolism and eliminated via the kidney. For many years SDMA has been considered inert and of little biological significance. However, a growing body of evidence now suggests this view is outdated and that circulating SDMA levels may, in fact, be intricately linked to endothelial dysfunction and vascular risk. In this review, we specifically examine SDMA within the context of cerebrovascular disease, with a particular focus on ischaemic stroke. We first discuss pre-clinical evidence supporting the notion that SDMA has effects on nitric oxide signalling, inflammation, oxidative stress, and HDL function. We then appraise the most recent clinical studies that explore the relationship between circulating SDMA and cerebrovascular risk factors, such as chronic kidney disease, hypertension, atrial fibrillation, and atherosclerosis, exploring whether any associations may arise due to the existence of shared risk factors. Finally, we consider the evidence that elevated circulating SDMA is linked to poor outcomes following ischaemic and haemorrhagic stroke. We draw upon pre-clinical insights into SDMA function to speculate how SDMA may not only be a marker of cerebrovascular disease but could also directly influence cerebrovascular pathology, and we highlight the pressing need for more mechanistic pre-clinical studies alongside adequately powered, longitudinal clinical studies to fully evaluate SDMA as a marker/mediator of disease.
Keywords: Symmetric dimethylarginine; cerebral ischemia; cerebrovascular disease; endothelial dysfunction; methylarginine.
© 2024 The Author(s).
Conflict of interest statement
The uthors declare that there are no competing interests associated with the manuscript.
Figures

References
-
- Turc G., Bhogal P., Fischer U., Khatri P., Lobotesis K., Mazighi M.et al. . (2019) European Stroke Organisation (ESO)- European Society for Minimally Invasive Neurological Therapy (ESMINT) guidelines on mechanical thrombectomy in acute ischemic stroke. J. Neurointerv. Surg. 11, 535–538 10.1136/neurintsurg-2018-014568 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources