

microRNA associated with hepatocyte injury and systemic inflammation may predict adverse outcomes in cirrhotic patients
- PMID: 39394217
- PMCID: PMC11470138
- DOI: 10.1038/s41598-024-72416-w
microRNA associated with hepatocyte injury and systemic inflammation may predict adverse outcomes in cirrhotic patients
Abstract
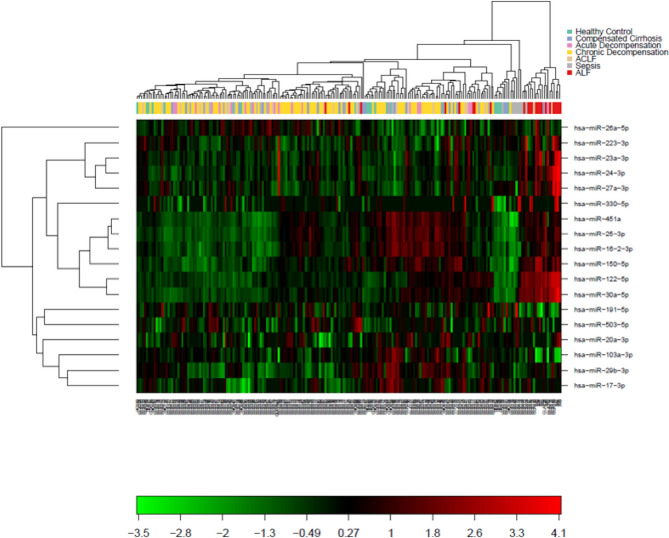
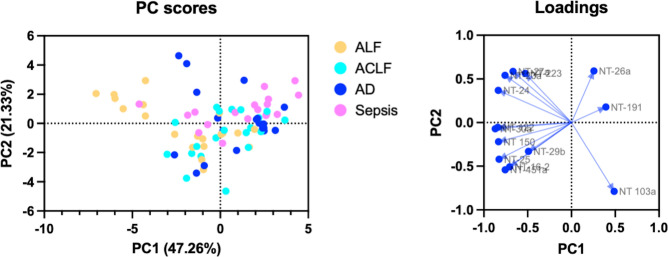
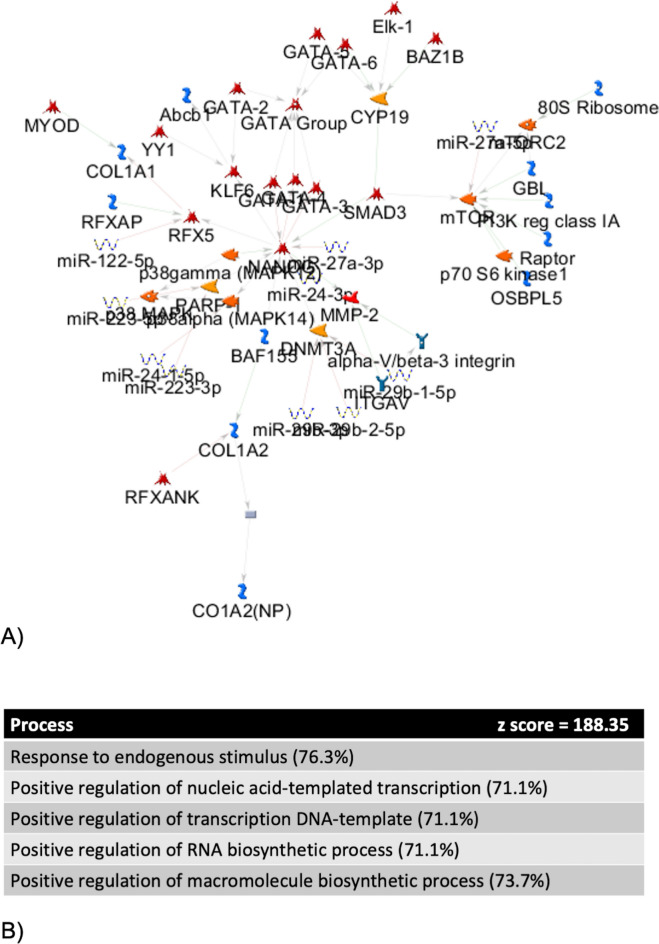
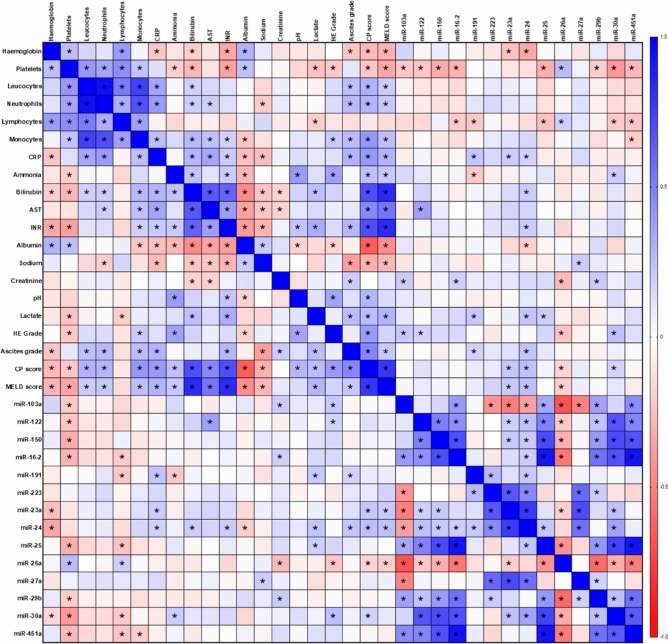
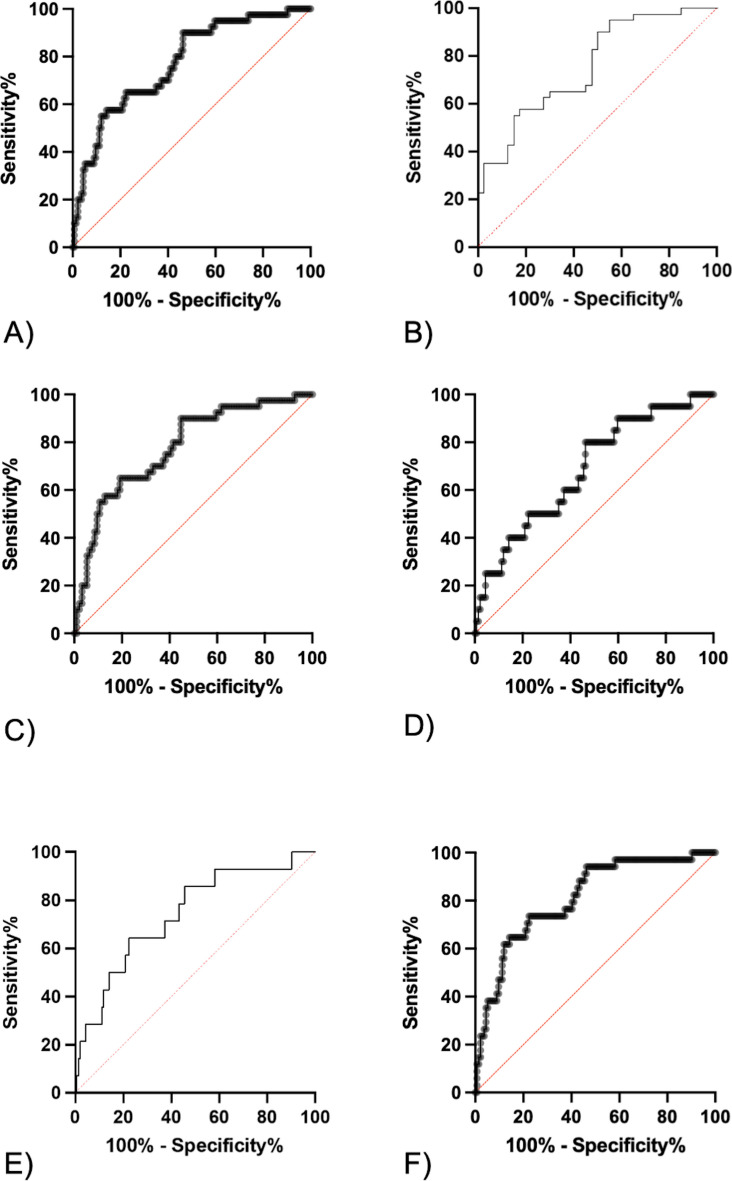
As the global prevalence of chronic liver disease continues to rise, the need to determine which patients will develop end-stage liver disease and require liver transplantation is increasingly important. However, current prognostic models perform sub-optimally. We aim to determine microRNA profiles associated with clinical decompensation and mortality/transplantation within 1 year. We examined microRNA expression profiles in plasma samples from patients across the spectrum of cirrhosis (n = 154), acute liver failure (ALF) (n = 22), sepsis (n = 20) and healthy controls (HC) (n = 20). We demonstrated that a microRNA-based model (miR-24 and -27a) associated with systemic inflammation differentiated decompensated cirrhosis states from compensated cirrhosis and HC (AUC 0.77 (95% CI 0.69-0.85)). 6 patients within the compensated cirrhosis group decompensated the subsequent year and their exclusion improved model performance (AUC 0.81 (95% CI 0.71-0.89)). miR-191 (associated with liver injury) predicted risk of mortality across the cohort when acutely decompensated and acute-on-chronic-liver failure patients were included. When they were excluded miR-24 (associated with systemic inflammation) predicted risk of mortality. Our findings demonstrate that microRNA associated with systemic inflammation and liver injury predict adverse outcomes in cirrhosis. miR-24 and -191 require further investigation as prognostic biomarkers and therapeutic targets for patients with liver disease.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Pimpin, L. et al. Burden of liver disease in Europe: Epidemiology and analysis of risk factors to identify prevention policies. J. Hepatol.69(3), 718–735 (2018). - PubMed
-
- Karlsen, T. H. et al. The EASL-Lancet Liver Commission: Protecting the next generation of Europeans against liver disease complications and premature mortality. Lancet399(10319), 61–116 (2022). - PubMed
-
- Trebicka, J. et al. The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology. J. Hepatol.73(4), 842–854 (2020). - PubMed
-
- Åberg, F. et al. Development and validation of a model to predict incident chronic liver disease in the general population: The CLivD score. J. Hepatol.77, 302–311 (2022). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
