

Brain hypoxia and metabolic crisis are common in patients with acute brain injury despite a normal intracranial pressure
- PMID: 39394442
- PMCID: PMC11470048
- DOI: 10.1038/s41598-024-75129-2
Brain hypoxia and metabolic crisis are common in patients with acute brain injury despite a normal intracranial pressure
Abstract
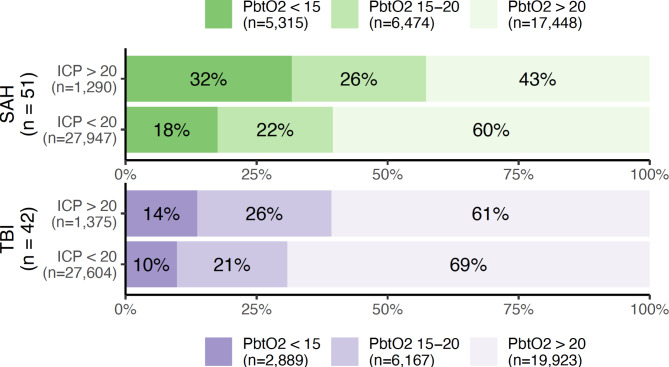
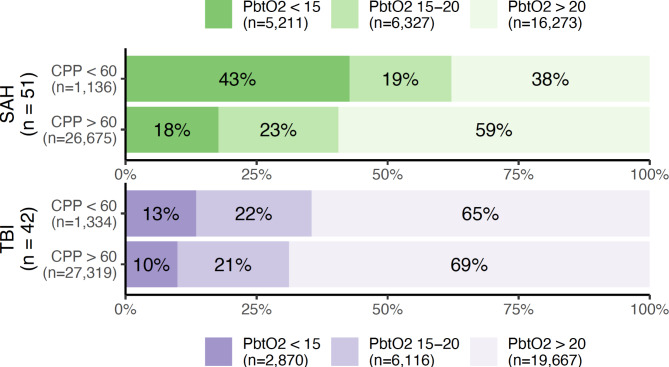
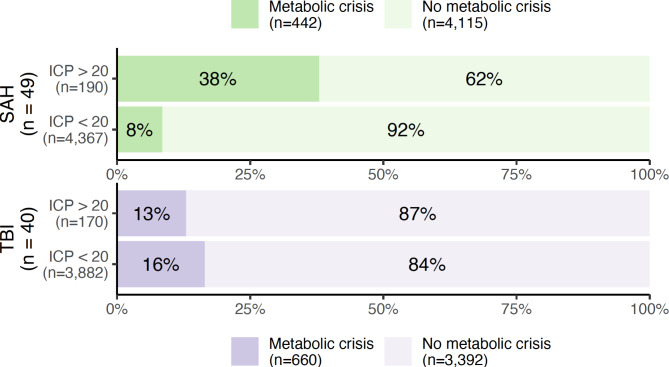
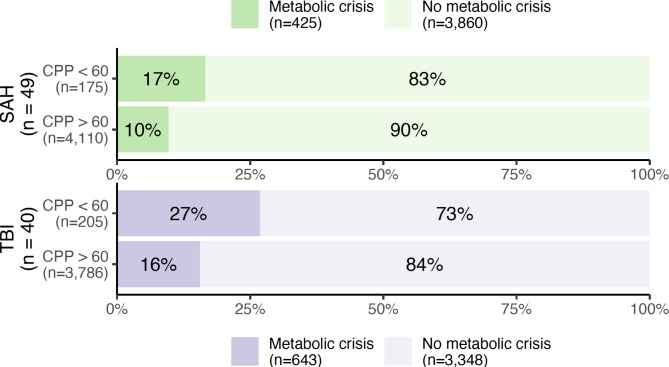
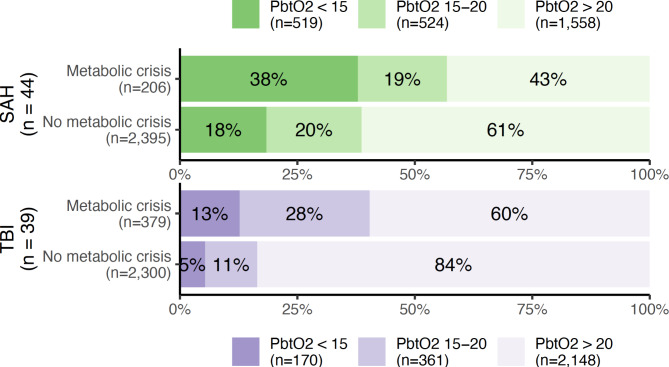
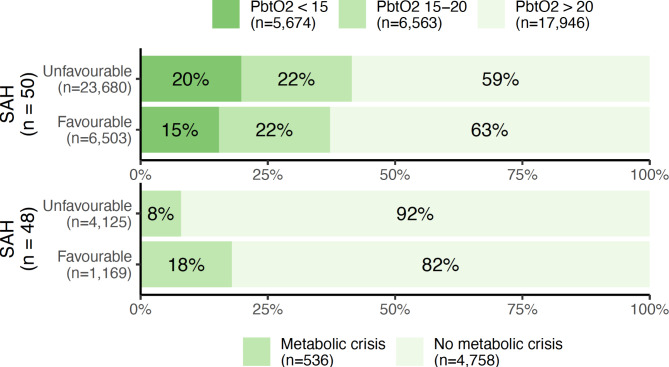
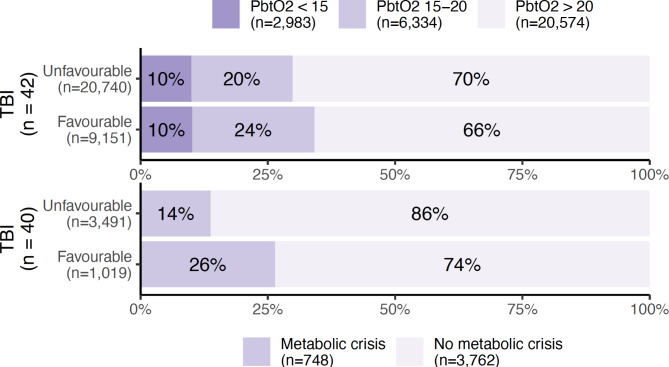
Patients with acute brain injury are vulnerable to secondary deterioration, which may go undetected by traditional monitoring. However, multimodal neuromonitoring of brain tissue oxygen tension (PbtO2) and energy metabolism may be able to detect such episodes. We report a retrospective, observational study of 94 patients with aneurysmal subarachnoid haemorrhage (SAH) or traumatic brain injury (TBI) who underwent multimodal neuromonitoring during admission. We examined the co-occurrence of pathological neuromonitoring values: elevated intracranial pressure (ICP, > 20 mmHg), inadequate cerebral perfusion pressure (CPP, < 60 mmHg), brain hypoxia (PbtO2 < 20 mmHg), and metabolic crisis (lactate/pyruvate ratio > 40 and a glucose level < 0.2 mmol/L in cerebral microdialysate). Mixed effects linear regression demonstrated significant associations between abnormal ICP/CPP, cerebral hypoxia and metabolic crisis. However, brain hypoxia occurred in 40% and 31% of observations in patients with SAH and TBI, respectively, despite normal concurrent values of ICP. Similarly, metabolic crisis was observed in 8% and 16% of measurements for SAH and TBI, respectively, despite a normal ICP. The pattern was identical for CPP. In conclusion, although all neuromonitoring variables are interrelated, brain hypoxia and metabolic crisis are common despite an absence of abnormalities in conventional monitoring. Multimodal neuromonitoring may help identify such episodes and guide individualised treatment.
Keywords: Brain hypoxia; Energy Metabolism; Intracranial hypertension; Intracranial pressure; Microdialysis; Oxygen; Subarachnoid hemorrhage; Traumatic brain Injury.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Werner, C. & Engelhard, K. Pathophysiology of traumatic brain injury. Br. J. Anaesth.. 99, 4–9. 10.1093/bja/aem131 (2007). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
