

TP53 mutation status and consensus molecular subtypes of colorectal cancer in patients from Rwanda
- PMID: 39394554
- PMCID: PMC11468329
- DOI: 10.1186/s12885-024-13009-8
TP53 mutation status and consensus molecular subtypes of colorectal cancer in patients from Rwanda
Abstract
Background: Mutations in the TP53 tumor suppressor gene are well-established drivers of colorectal cancer (CRC) development. However, data on the prevalence of TP53 variants and their association with consensus molecular subtype (CMS) classification in patients with CRC from Rwanda are currently lacking. This study addressed this knowledge gap by investigating TP53 mutation status concerning CMS classification in a CRC cohort from Rwanda.
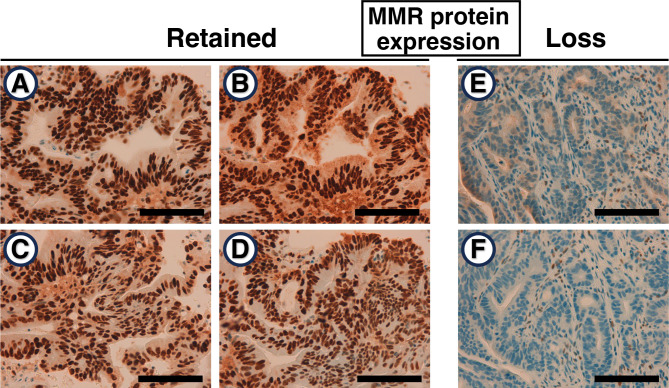
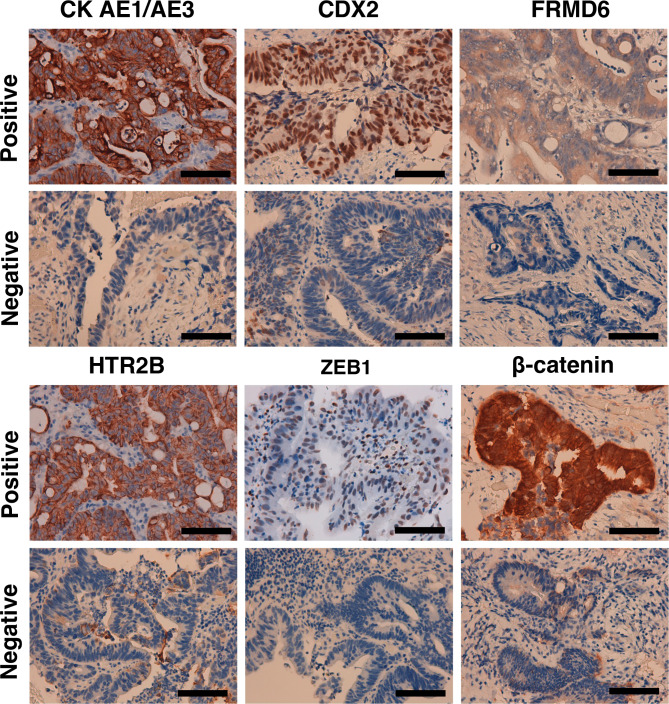
Methods: Formalin-fixed paraffin-embedded (FFPE) tissue blocks were obtained from 51 patients with CRC at the University Teaching Hospital of Kigali, Rwanda. Exons 4 to 11 and their flanking intron-exon boundaries in the TP53 gene were sequenced using Sanger sequencing to identify potential variants. The recently established immunohistochemistry-based classifier was employed to determine the CMS of each tumor.
Results: Sequencing analysis of cancerous tissue DNA revealed TP53 pathogenic variants in 23 of 51 (45.1%) patients from Rwanda. These variants were predominantly missense types (18/23, 78.3%). The most frequent were c.455dup (p.P153Afs*28), c.524G > A (p.R175H), and c.733G > A (p.G245S), each identified in three tumors. Trinucleotide sequence context analysis of the 23 mutations (20 of which were single-base substitutions) revealed a predominance of the [C > N] pattern among single-base substitutions (SBSs) (18/20; 90.0%), with C[C > T]G being the most frequent mutation (5/18, 27.8%). Furthermore, pyrimidine bases (C and T) were preferentially found at the 5' flanking position of the mutated cytosine (13/18; 72.2%). Analysis of CMS subtypes revealed the following distribution: CMS1 (microsatellite instability-immune) (6/51, 11.8%), CMS2 (canonical) (28/51, 54.9%), CMS3 (metabolic) (9/51, 17.6%), and CMS4 (mesenchymal) (8/51, 15.7%). Interestingly, the majority of TP53 variants were in the CMS2 subgroup (14/23; 60.1%).
Conclusion: Our findings indicate a high frequency of TP53 variants in CRC patients from Rwanda. Importantly, these variants are enriched in the CMS2 subtype. This study, representing the second investigation into molecular alterations in patients with CRC from Rwanda and the first to explore TP53 mutations and CMS classification, provides valuable insights into the molecular landscape of CRC in this understudied population.
Keywords: TP53; Africa; Colorectal cancer; Consensus molecular subtypes; Mismatch repair; Mutation pattern; Mutation spectrum; Rwanda.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer [Internet]. 2024 [cited 2024 Aug 18]. https://gco.iarc.who.int/today
-
- Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. [Internet]. 2024 [cited 2024 Apr 10]. https://gco.iarc.who.int/today
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
