

External validation of dementia prediction models in Black or African American and White older adults: A longitudinal population-based study in the United States
- PMID: 39394865
- PMCID: PMC11567852
- DOI: 10.1002/alz.14280
External validation of dementia prediction models in Black or African American and White older adults: A longitudinal population-based study in the United States
Abstract
Introduction: Identifying people at high risk of Alzheimer's disease (AD) dementia allows for timely intervention, which, if successful, will result in preventing or delaying the onset of the disease.
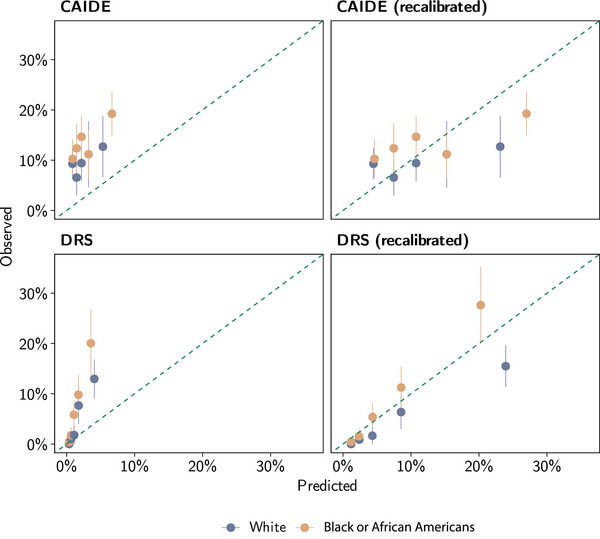
Methods: Utilizing data from the Chicago Health and Aging Project (CHAP; n = 2130), we externally evaluated four risk-prediction models for AD dementia, including Cardiovascular Risk Factors, Aging, and Dementia (CAIDE), Australian National University Alzheimer's Disease Risk Index (ANU-ADRI), Brief Dementia Screening Indicator (BDSI), and Dementia Risk Score (DRS), in Black or African American and White adults.
Results: BDSI had the highest discriminate abilities for AD dementia (c-statistics of 0.79 in Black and 0.77 in White adults), followed by ANU-ADRI, within the age range and follow-up period of the original development cohort. CAIDE had the lowest discriminating power (c-statistic ≤0.55). With increasing follow-up periods (i.e., 10-15 years), the discrimination abilities for all models declined.
Discussion: Because of racial disparities in AD dementia and longer preclinical and prodromal stages of disease development, race-specific models are needed to predict AD risk over 10 years.
Highlights: Utilizing risk-prediction models to identify individuals at higher risk of Alzheimer's disease (AD) dementia could benefit clinicians, patients, and policymakers. Clinicians could enroll high-risk individuals in clinical trials to test new risk-modifiable treatments or initiate lifestyle modifications, which, if successful, would slow cognitive decline and delay the onset of the disease. Current risk-prediction models had good discriminative power during the first 6 years of follow-up but decreased with longer follow-up time. Acknowledging the longer preclinical phase of AD dementia development and racial differences in dementia risk, there is a need to develop race-specific risk-prediction models that can predict 10 or 20 years of risk for AD and related dementias.
Keywords: Alzheimer's disease; Black or African American; White; dementia; risk assessment; validation.
© 2024 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
Klodian Dhana is funded by the Alzheimer's Association and National Institutes of Health (NIH) research grants and reports no conflicts of interest. Lisa L. Barnes, Todd Beck, Anisa Dhana, Xiaoran Liu, Pankaja Desai, Ted K.S. Ng, Denis A. Evans, and Kumar B. Rajan report no conflicts of interest. Author disclosures are available in the supporting information.
Figures
References
-
- Dhana K, Beck T, Desai P, Wilson RS, Evans DA, Rajan KB. Prevalence of Alzheimer's disease dementia in the 50 US states and 3142 counties: a population estimate using the 2020 bridged‐race postcensal from the national center for health statistics. Alzheimers Dementia. 2023;19(10):4388‐4395. doi: 10.1002/alz.13081 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
