

Targeted delivery of napabucasin with radiotherapy improves outcomes in diffuse midline glioma
- PMID: 39394920
- PMCID: PMC11889722
- DOI: 10.1093/neuonc/noae215
Targeted delivery of napabucasin with radiotherapy improves outcomes in diffuse midline glioma
Abstract
Background: Diffuse midline glioma (DMG) is the most aggressive primary brain tumor in children. All previous studies examining the role of systemic agents have failed to demonstrate a survival benefit; the only standard of care is radiation therapy (RT). Successful implementation of radiosensitization strategies in DMG remains an essential and promising avenue of investigation. We explore the use of Napabucasin, an NAD(P)H quinone dehydrogenase 1 (NQO1)-bioactivatable reactive oxygen species (ROS)-inducer, as a potential therapeutic radiosensitizer in DMG.
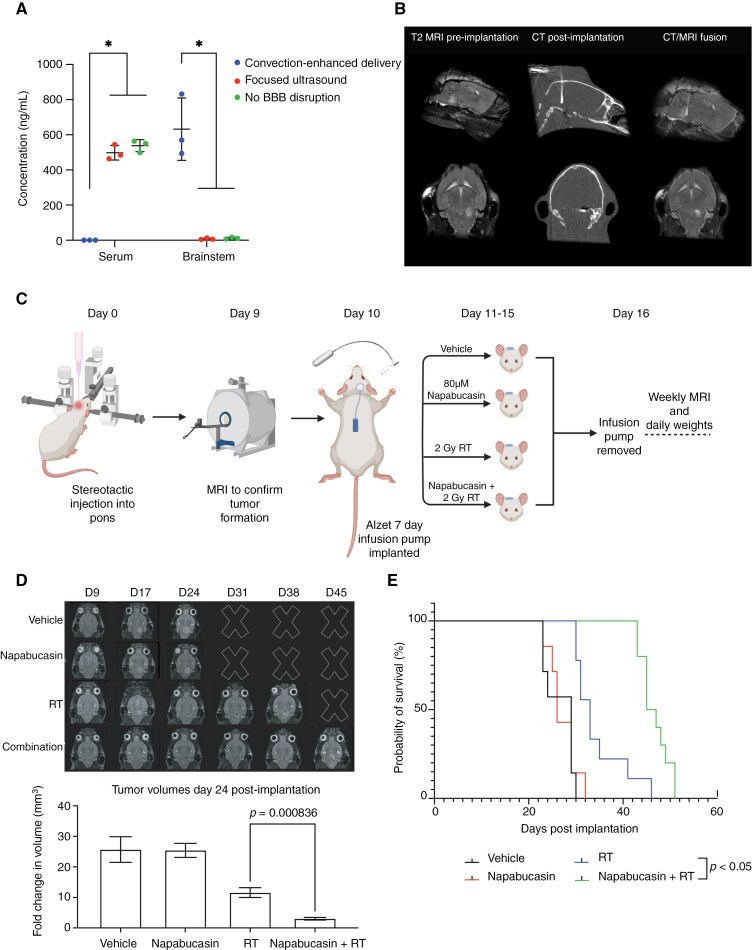
Methods: In this study, we conduct in vitro and in vivo assays using patient-derived DMG cultures to elucidate the mechanism of action of Napabucasin and its radiosensitizing properties. As penetration of systemic therapy through the blood-brain barrier (BBB) is a significant limitation to the success of DMG therapies, we explore focused ultrasound (FUS) and convection-enhanced delivery (CED) to overcome the BBB and maximize therapeutic efficacy.
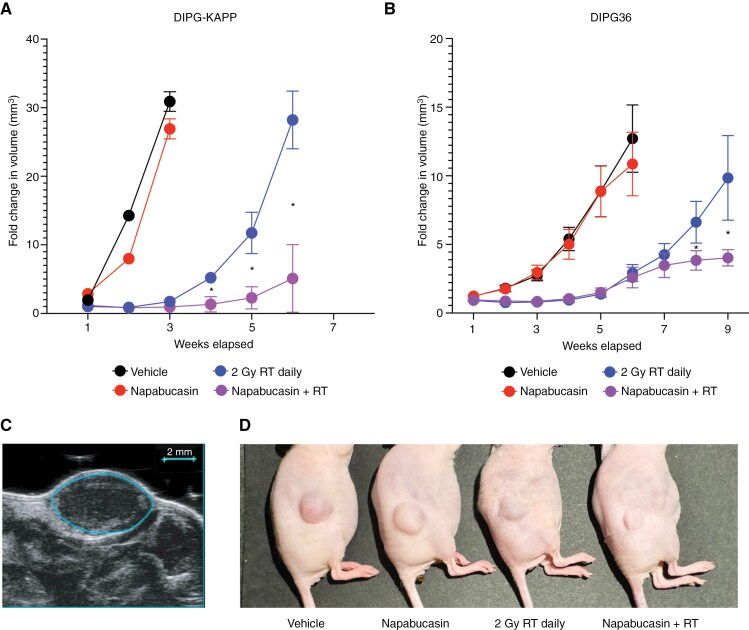
Results: Napabucasin is a potent ROS-inducer and radiosensitizer in DMG, and treatment-mediated ROS production and cytotoxicity are dependent on NQO1. In subcutaneous xenograft models, combination therapy with RT improves local control. After optimizing targeted drug delivery using CED in an orthotopic mouse model, we establish the novel feasibility and survival benefit of CED of Napabucasin concurrent with RT.
Conclusions: As nearly all DMG patients will receive RT as part of their treatment course, our validation of the efficacy of radiosensitizing therapy using CED to prolong survival in DMG opens the door for exciting novel studies of alternative radiosensitization strategies in this devastating disease while overcoming limitations of the BBB.
Keywords: blood-brain barrier; convection-enhanced drug delivery; diffuse midline glioma; focused ultrasound; radiosensitization.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Dr. Califano is founder, equity holder, and consultant of DarwinHealth Inc., a company that has licensed some of the algorithms used in this manuscript from Columbia University. Columbia University is also an equity holder in DarwinHealth Inc. US patent number 10,790,040 has been awarded related to this work, and has been assigned to Columbia University with Dr. Califano as an inventor. Lorenzo Tomassoni is an employee of DarwinHealth Inc.
Figures




References
-
- Hankinson TC, Campagna EJ, Foreman NK, Handler MH.. Interpretation of magnetic resonance images in diffuse intrinsic pontine glioma: A survey of pediatric neurosurgeons. J Neurosurg Pediatr. 2011;8(1):97–102. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
