

Real-world assessment of immunogenicity in immunocompromised individuals following SARS-CoV-2 mRNA vaccination: a two-year follow-up of the prospective clinical trial COVAXID
- PMID: 39395230
- PMCID: PMC11663764
- DOI: 10.1016/j.ebiom.2024.105385
Real-world assessment of immunogenicity in immunocompromised individuals following SARS-CoV-2 mRNA vaccination: a two-year follow-up of the prospective clinical trial COVAXID
Abstract
Background: Immunocompromised patients with primary and secondary immunodeficiencies have shown impaired responses to SARS-CoV-2 mRNA vaccines, necessitating recommendations for additional booster doses. However, longitudinal data reflecting the real-world impact of such recommendations remains limited.
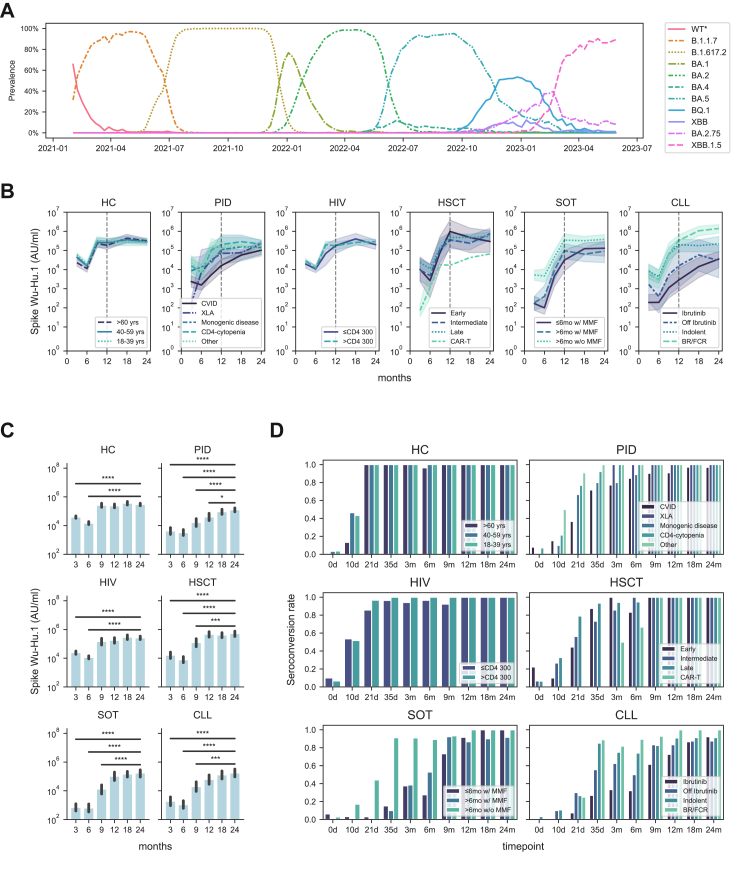
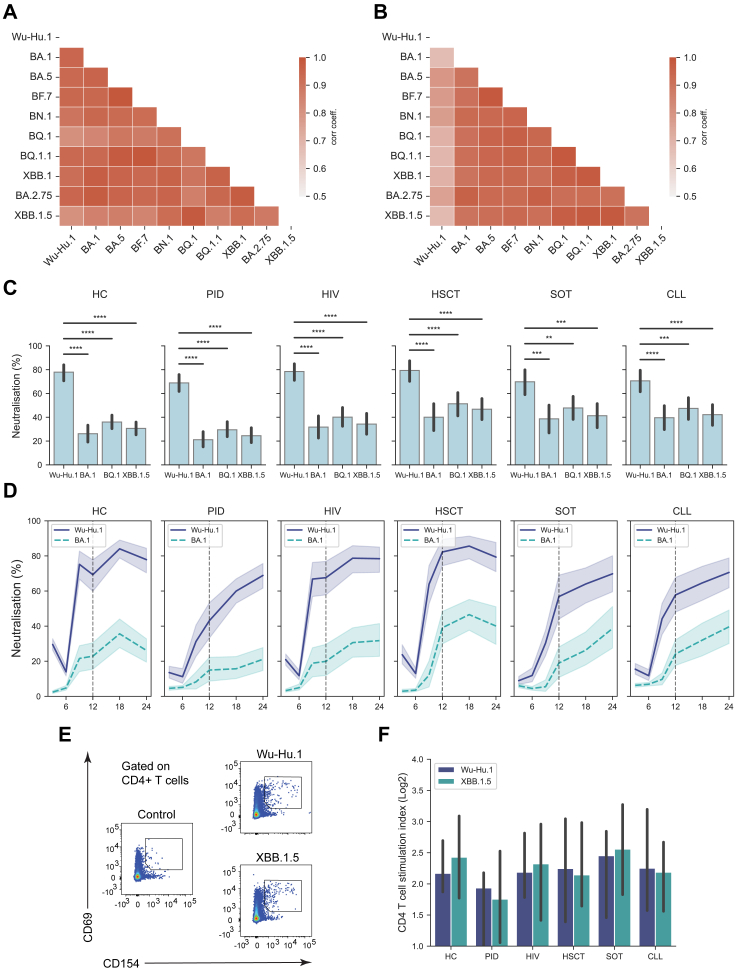
Methods: This study represents a two-year follow-up of the COVAXID clinical trial, where 364 of the original 539 subjects consented to participate. 355 individuals provided blood samples for evaluation of binding antibody (Ab) titers and pseudo-neutralisation capacity against both the ancestral SARS-CoV-2 strain and prevalent Omicron variants. T cell responses were assessed in a subset of these individuals. A multivariate analysis determined the correlation between Ab responses and the number of vaccine doses received, documented infection events, immunoglobulin replacement therapy (IGRT), and specific immunosuppressive drugs. The original COVAXID clinical trial was registered in EudraCT (2021-000175-37) and clinicaltrials.gov (NCT04780659).
Findings: Several of the patient groups that responded poorly to the initial primary vaccine schedule and early booster doses presented with stronger immunogenicity-related responses including binding Ab titres and pseudo-neutralisation at the 18- and 24-month sampling time point. Responses correlated positively with the number of vaccine doses and infection. The vaccine response was blunted by an immunosuppressive state due to the underlying specific disease and/or to specific immunosuppressive treatment.
Interpretation: The study results highlight the importance of continuous SARS-CoV-2 vaccine booster doses in building up and sustaining Ab responses in specific immunocompromised patient populations.
Funding: The present studies were supported by the European Research Council, Karolinska Institutet, Knut and Alice Wallenberg Foundation, Nordstjernan AB, Region Stockholm, and the Swedish Research Council.
Keywords: COVID-19; Chronic lymphocytic leukemia; Clinical study; HIV; Hematopoietic stem cell transplantation; Primary immunodeficiency disease; SARS-CoV-2; Solid organ transplantation; mRNA vaccine.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests PB has received honoraria from Takeda and Novartis for educational lectures not directly relevant to this work. SM has received honoraria from Celgene/BMS, Novartis, Gilead/Kite, and DNA Prime for lectures and educational events, and as a member and/or head of data safety monitoring boards from Miltenyi and Immunicum not directly relevant to this work. CIES has received financial support from Moderna for work not directly relevant to this work. KL has received financial support from Moderna for work not directly relevant to this work. PL has received grants from Pfizer, MSD, and personal fees from Takeda, AiCuris, and OctaPharma, not directly relevant to this work. MB has served as a consultant and received honoraria from Oxford Immunotech, Gilead, MSD, BMS, Pfizer, and Mabtech, not relevant to this work. SA has received honoraria for lectures from Gilead with payment to Karolinska University Hospital and Karolinska Institutet, participated in advisory boards/consultation for Gilead and Ribocure with waived compensation not directly related to this work, and reports grants from the Swedish Research Council on COVID-19 vaccination. HGL received honoraria from Sanofi and Vycellix for consultation not relevant to this work, served on the UK-CIC Oversight Committee, led the Karolinska Institutet COVID-19 vaccine group, and is on the scientific advisory group for the International Vaccine Institute. All other authors declare no potential or actual conflict of interest to the work presented in this paper.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
