

Immune microenvironment modulation following neoadjuvant therapy for oesophageal adenocarcinoma: a translational analysis of the DEBIOC clinical trial
- PMID: 39395265
- PMCID: PMC11693431
- DOI: 10.1016/j.esmoop.2024.103930
Immune microenvironment modulation following neoadjuvant therapy for oesophageal adenocarcinoma: a translational analysis of the DEBIOC clinical trial
Abstract
Background: The Dual Erb B Inhibition in Oesophago-gastric Cancer (DEBIOC) trial reported an acceptable safety profile for neoadjuvant oxaliplatin and capecitabine (Xelox) ± AZD8931 in oesophageal adenocarcinoma (OAC) but limited efficacy. We evaluated the impact of neoadjuvant Xelox ± AZD8931, a novel small-molecule inhibitor with equipotent activity against epidermal growth factor receptor (EGFR), human epidermal growth factor receptor (HER)2 and HER3, on biological pathways using a unique software-driven solution.
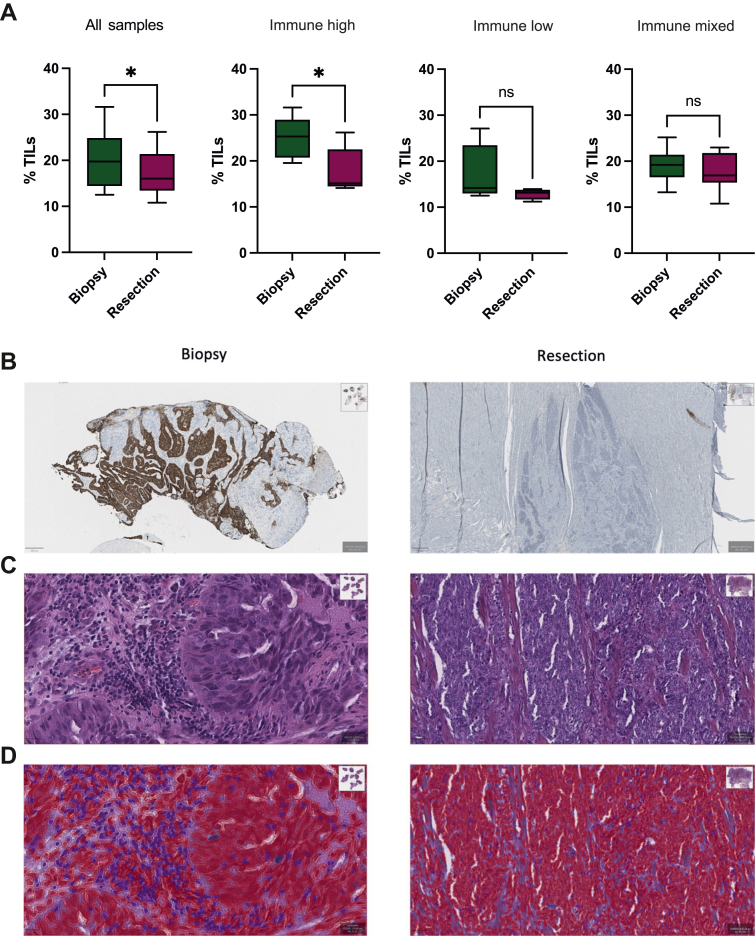
Patients and methods: Transcriptomic profiles from 25 pre-treatment formalin-fixed paraffin-embedded OAC biopsies and 18 matched resection specimens, treated with Xelox + AZD8931 (n = 16) and Xelox alone (n = 9), were analysed using the Almac claraT total mRNA report analysing 92 gene signatures, 100 unique single-gene drug targets and 7337 single genes across 10 hallmarks of cancer. Gene-set enrichment analysis (GSEA) was utilised to investigate pathways governing pathological response. Tumour-infiltrating lymphocytes (TILs) were assessed digitally using the QuPath software.
Results: Hierarchical clustering identified three molecular subgroups classified by activation of innate immune signalling. The immune-high subgroup was associated with HER2 positivity, increased pathological response and a marked reduction in immune signalling and TILs following neoadjuvant therapy. The immune-low cluster was predominantly HER2/EGFR-negative, and EGFR positivity was associated with the immune-mixed subgroup. Treatment with neoadjuvant therapy induced common resistance mechanisms, such as angiogenesis and epithelial-mesenchymal transition signalling, and a reduction in DNA repair signatures. Addition of AZD8931 was associated with reduction of expression of EGFR, HER2 and AKT pathways and also promoted an immunosuppressive microenvironment. GSEA showed that patients with a pathological response to treatment had increased immune signalling, whereas non-responders to neoadjuvant therapy were enriched for nucleotide repair and cellular growth through the action of E2F transcription factors.
Conclusion: OAC may be subdivided into three immune-related subgroups which undergo modulation in response to neoadjuvant therapy with marked suppression of the immune microenvironment in HER2-positive/immune-high tumours.
Keywords: AZD8931; adenocarcinoma; gene expression signature; oesophageal cancer.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures






References
-
- Morgan E., Soerjomataram I., Gavin A.T., et al. International trends in oesophageal cancer survival by histological subtype between 1995 and 2014. Gut. 2020 gutjnl-2020-321089. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
