

Dynamic choice HIV prevention with cabotegravir long-acting injectable in rural Uganda and Kenya: a randomised trial extension
- PMID: 39395424
- PMCID: PMC11753513
- DOI: 10.1016/S2352-3018(24)00235-2
Dynamic choice HIV prevention with cabotegravir long-acting injectable in rural Uganda and Kenya: a randomised trial extension
Erratum in
-
Correction to Lancet HIV 2024; 11: e736-45.Lancet HIV. 2024 Dec;11(12):e805. doi: 10.1016/S2352-3018(24)00302-3. Epub 2024 Nov 6. Lancet HIV. 2024. PMID: 39521014 No abstract available.
Abstract
Background: HIV infections are ongoing globally despite efficacious biomedical prevention options. We sought to determine whether an HIV prevention package providing choice of daily pills or long-acting injectable cabotegravir and opportunities to change prevention options could increase biomedical prevention coverage and reduce new HIV infections.
Methods: This study was an extension of three randomised trials that used SEARCH dynamic choice HIV prevention to recruit adults (aged ≥15 years) at risk for HIV from antenatal, outpatient, and community settings in rural Uganda and Kenya. In this 48-week open-label extension, participants maintained their original (1:1) randomisation group; the option to choose cabotegravir long-acting injectable was added for intervention participants. Inclusion criteria for the extension were previous enrolment in a SEARCH dynamic choice HIV prevention trial, negative HIV rapid test, and residence in study region. The intervention provided person-centred choice of oral pre-exposure prophylaxis (PrEP) or post-exposure HIV prophylaxis (PEP) or cabotegravir long-acting injectable, with the option to switch according to participant preference. The control provided standard-of-care access to oral PrEP and PEP, but not cabotegravir long-acting injectable. Biomedical prevention coverage (proportion of follow-up covered by oral PrEP, PEP, or cabotegravir long-acting injectable; primary outcome) and HIV incidence (secondary outcome) were compared between groups using targeted minimum loss-based estimation. The trial (NCT05549726) is closed to recruitment.
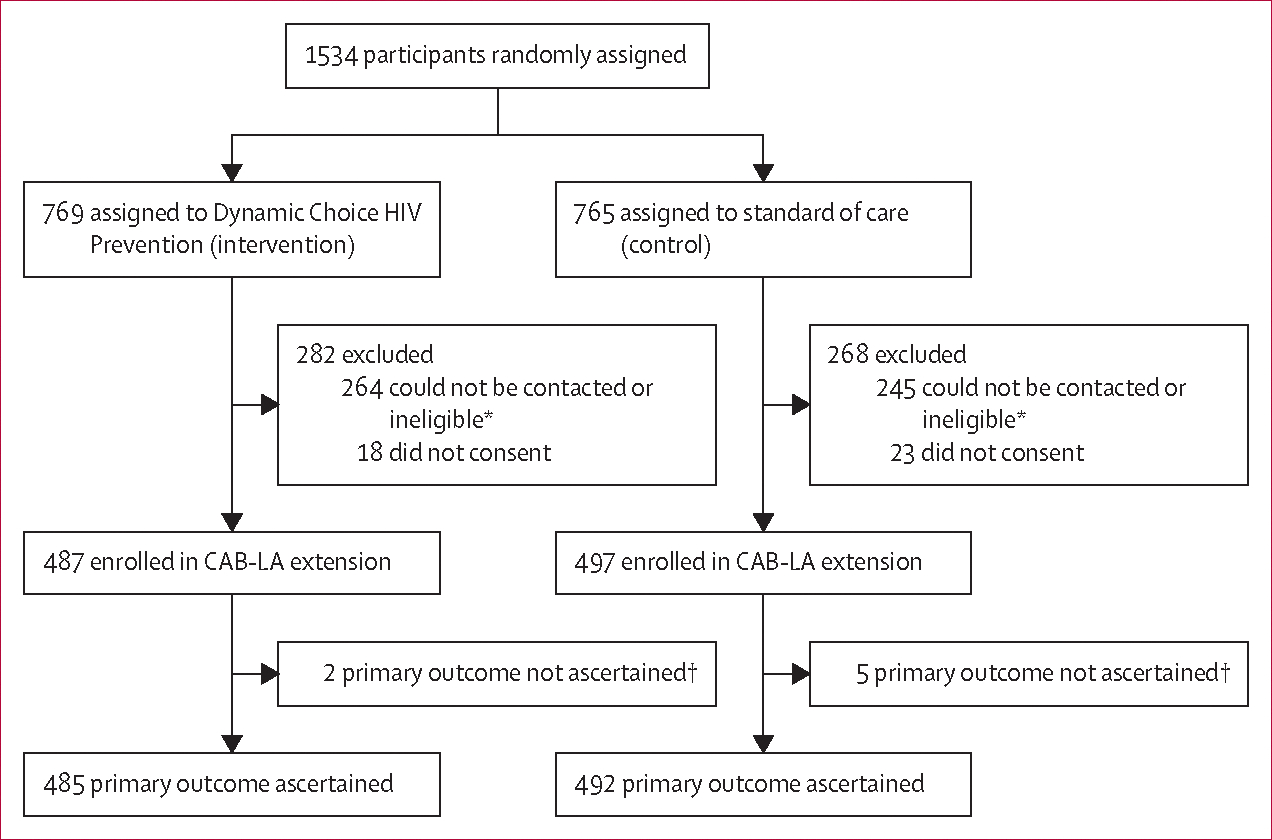
Findings: Of 1534 participants initially randomly assigned (from April 15, 2021 to Sept 29, 2022), 984 (487 in the intervention group and 497 in the standard-of-care group) reconsented to the extension (from Jan 2 to March 3, 2023). The mean proportion of follow-up covered by biomedical HIV prevention was 69·7% (95% CI 64·9-74·5) in the intervention group versus 13·3% (10·2-16·3) in the standard-of-care group, corresponding to an absolute difference of 56·4 percentage points (95% CI 50·8-62·1; p<0·0001). The intervention significantly improved coverage across prespecified subgroups (sex and age groups). During the study, 274 (56%) of 485 intervention participants used cabotegravir long-acting injectable, 255 (53%) used oral PrEP, and ten (2%) used PEP. Among cabotegravir long-acting injectable initiators, 118 (43%) of 274 were not previously using oral PrEP or PEP. There were seven incident HIV infections in 390 person-years of follow-up in the standard-of-care group and no infections in 400 person-years of follow-up in the intervention group (incidence rate difference per 100 person-years 1·8, 95% CI 0·4-3·2; p=0·014).
Interpretation: Offering people the choice of HIV biomedical prevention options including cabotegravir long-acting injectable in a flexible model can increase prevention coverage and reduce incident HIV infections. HIV programmes should support dynamic choice HIV prevention programmes that include effective oral and injectable long-acting products.
Funding: National Institutes of Health.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests DVH reports funding from the US National Institutes of Health (NIH). MB is a salaried employee of the NIH, serving as Medical Officer for this study as part of her covered duties, which included assisting with protocol development and review, project oversight, and review of manuscripts. AR is a shareholder of GlaxoSmithKline. ViiV Healthcare provided CAB-LA for the study. All other authors declare no competing interests related to this work.
Figures


References
-
- Joint United Nations Programme on HIV/AIDS. The urgency of now: AIDS at a crossroads. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS), 2024. https://crossroads.unaids.org/wp-content/uploads/2024/07/GAU-2024-Full-r... (accessed Jan 8, 2024).
-
- Landovitz RJ, Scott H, Deeks SG. Prevention, treatment and cure of HIV infection. Nat Rev Microbiol 2023; 21: 657–70. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
