

Endovascular thrombectomy after anterior circulation large vessel ischemic stroke: an updated meta-analysis
- PMID: 39396031
- PMCID: PMC11475204
- DOI: 10.1186/s13643-024-02670-6
Endovascular thrombectomy after anterior circulation large vessel ischemic stroke: an updated meta-analysis
Abstract
Background: Endovascular thrombectomy (EVT) has emerged as the established standard of care for the treatment of anterior circulation large-vessel occlusion (LVO). However, its benefits remain unclear in specific patient populations. Herein, we present an updated systematic review and meta-analysis aimed at thoroughly assessing the effectiveness and safety of combining EVT with medical treatment (MT) compared with MT alone.
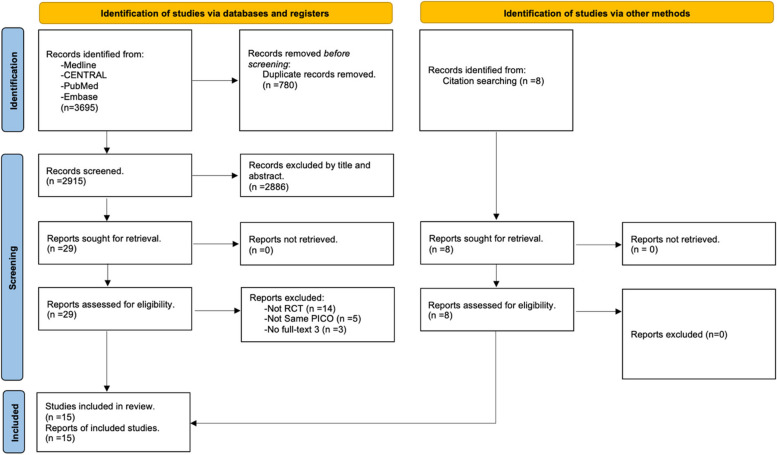
Methods: This systematic review was performed in accordance with the PRISMA guideline. The MEDLINE, Embase, and Cochrane databases were systematically searched to identify relevant articles published until December 30, 2023. The inclusion criteria restricted articles to randomized clinical trials (RCTs). We pooled odds ratios (OR) and their respective 95% confidence intervals (CIs).
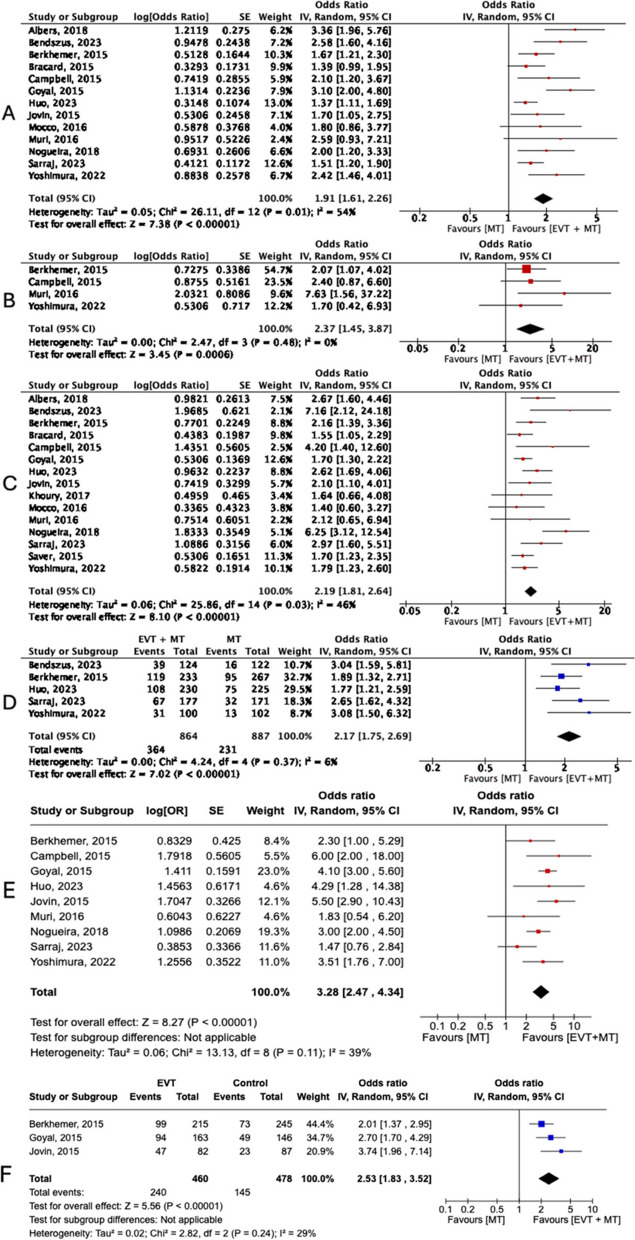
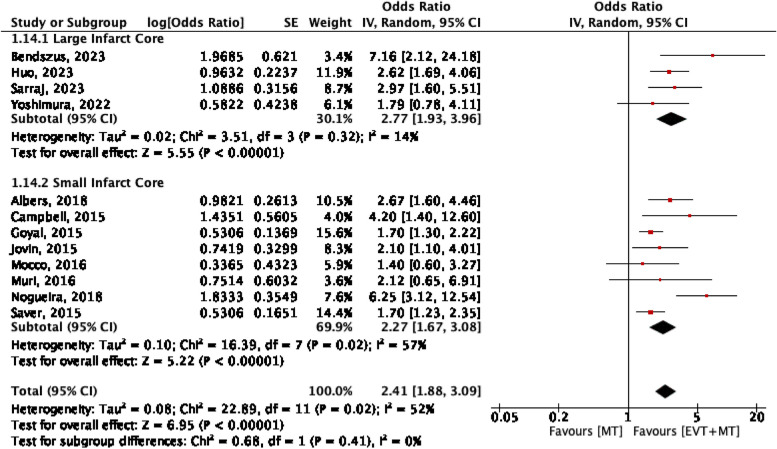
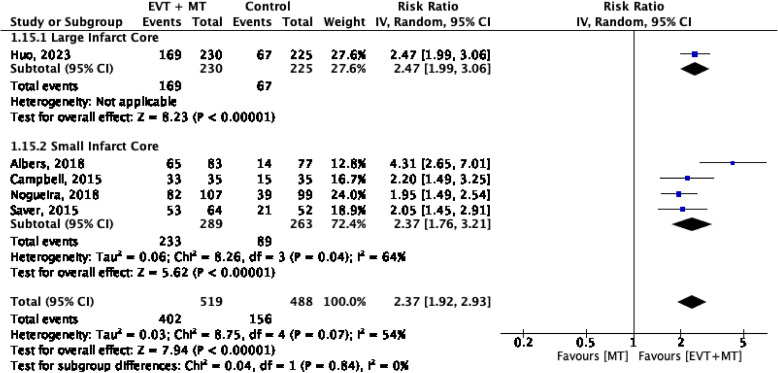
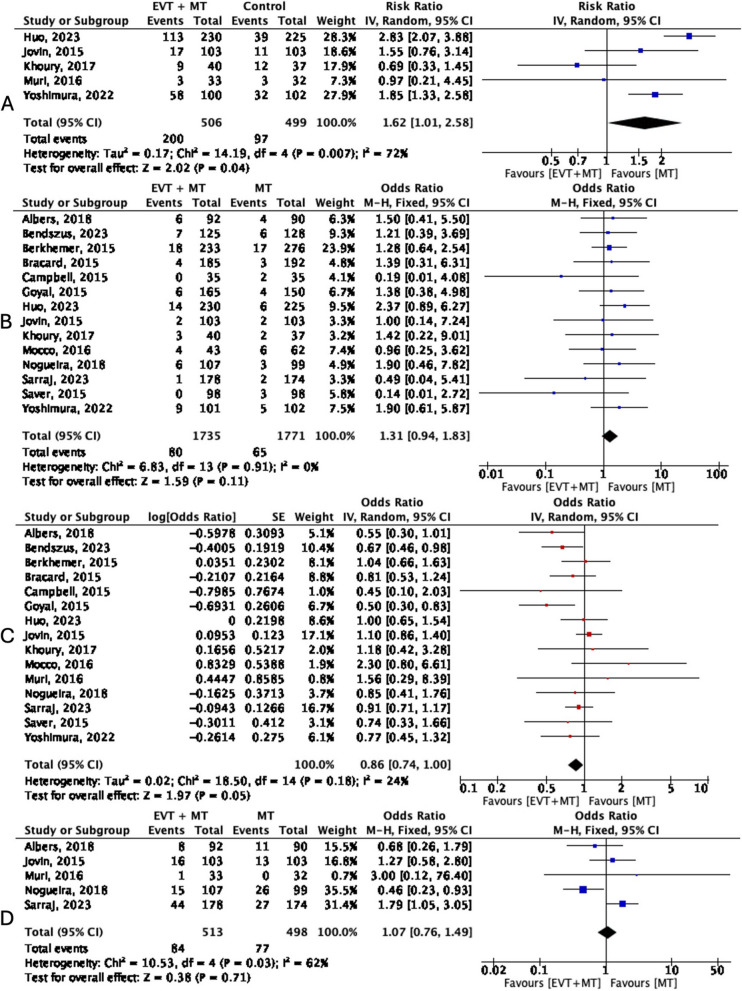
Results: Fifteen RCTs involving 3897 patients were included in the study. EVT plus MT was associated with a significant reduction in disability at 90 days (OR = 1.91, [1.61-2.26]), improved functional independence (modified Rankin Scale [mRS] 0-2) (OR = 2.19 [1.81-2.64]), excellent functional outcomes (mRS 0-1) (OR = 2.37, [1.45-3.87]), improved independent ambulation (mRS 0-3) (OR = 2.17, [1.75-2.69]), and higher rates of partial/complete recanalization (OR = 2.18, [1.66-2.87] compared with EVT. Efficacy outcomes for both large and small infarct cores were statistically favorable following EVT. Safety outcomes showed comparable rates, except for intracerebral and subarachnoid hemorrhage, which favored MT alone.
Conclusion: This meta-analysis supports the use of EVT plus MT as the standard of care for acute ischemic stroke patients with LVO of any infarct core size, as it offers substantial improvements in functional outcomes and recanalization. Safety considerations, particularly the risk of hemorrhage, warrant careful patient selection. These findings provide valuable insights for optimizing stroke management protocols and enhancing patient outcomes.
Keywords: Anterior circulation; Endovascular thrombectomy; Large vessel ischemic stroke; Meta-analysis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics–2015 update: a report from the American Heart Association. Circulation. 2015;131(4):29–322. 10.1161/CIR.0000000000000152. - DOI - PubMed
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, Dávalos A, Majoie CB, van der Lugt A, de Miquel MA, Donnan GA, Roos YB, Bonafe A, Jahan R, Diener HC, van den Berg LA, Levy EI, Berkhemer OA, Pereira VM, Rempel J, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet (London, England). 2016;387(10029):1723–31. 10.1016/S0140-6736(16)00163-X. - DOI - PubMed
-
- Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, Demaerschalk BM, Khatri P, McMullan PW Jr, Qureshi AI, Rosenfield K, Scott PA, Summers DR, Wang DZ, Wintermark M, Yonas H. American Heart Association Stroke Council, Council on Cardiovascular Nursing, Council on Peripheral Vascular Disease, & Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(3):870–947. 10.1161/STR.0b013e318284056a. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, Yan B, Dowling RJ, Parsons MW, Oxley TJ, Wu TY, Brooks M, Simpson MA, Miteff F, Levi CR, Krause M, Harrington TJ, Faulder KC, Steinfort BS, Priglinger M. EXTEND-IA Investigators. Endovascular therapy for ischemic stroke with perfusion-imaging selection. New England J Med. 2015;372(11):1009–1018. 10.1056/NEJMoa1414792. - PubMed
-
- Sarraj A, Hassan AE, Abraham MG, Ortega-Gutierrez S, Kasner SE, Hussain MS, Chen M, Blackburn S, Sitton CW, Churilov L, Sundararajan S, Hu YC, Herial NA, Jabbour P, Gibson D, Wallace AN, Arenillas JF, Tsai JP, Budzik RF, Hicks WJ, et al. Trial of endovascular thrombectomy for large ischemic strokes. New England J Med. 2023;388(14):1259–71. 10.1056/NEJMoa2214403. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
