

A comparative study of postadrenalectomy hyperuricemia and renal impairment in patients with unilateral primary aldosteronism: does histopathology subtype matter?
- PMID: 39396977
- PMCID: PMC11472553
- DOI: 10.1186/s12882-024-03750-4
A comparative study of postadrenalectomy hyperuricemia and renal impairment in patients with unilateral primary aldosteronism: does histopathology subtype matter?
Abstract
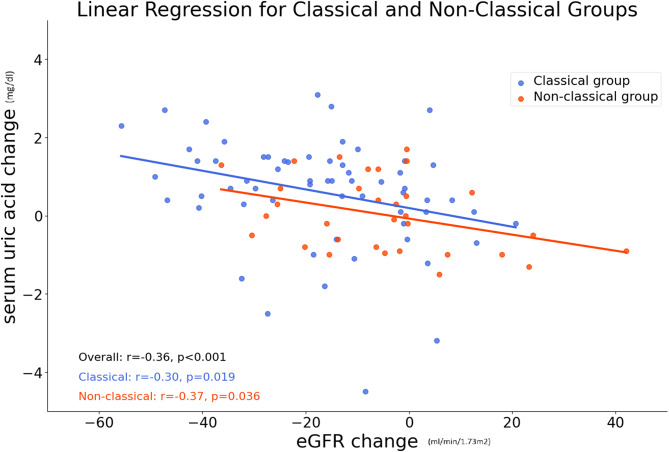
Background: Primary aldosteronism (PA), which is present in 5-18% of hypertensive patients, is a leading cause of secondary hypertension. Adrenalectomy is often recommended for patients with unilateral primary aldosteronism (uPA), yielding good long-term outcomes. PA patients without hyperuricemia and chronic renal failure before adrenalectomy were enrolled in this cohort study. Serum uric acid (SUA) and renal filtration were measured one year post-adrenalectomy. Their relationships with pathologic features, histopathological subtype (classical or nonclassical (HISTALDO consensus)), and vessel stiffness were explored. The aim of this cohort study is to evaluate the correlation between post-adrenalectomy serum uric acid (SUA) levels and estimated glomerular filtration rate (eGFR) with the pathologic features delineated by the HISTALDO consensus. Additionally, the study seeks to assess the impact of these biochemical markers on peripheral vessel stiffness and brachial-ankle pulse wave velocity (baPWV) at a one-year follow-up visit.
Methods: This prospective cohort study included patients (N = 100) diagnosed with uPA who underwent adrenalectomy from Jan 1, 2007 to Dec 31, 2022.
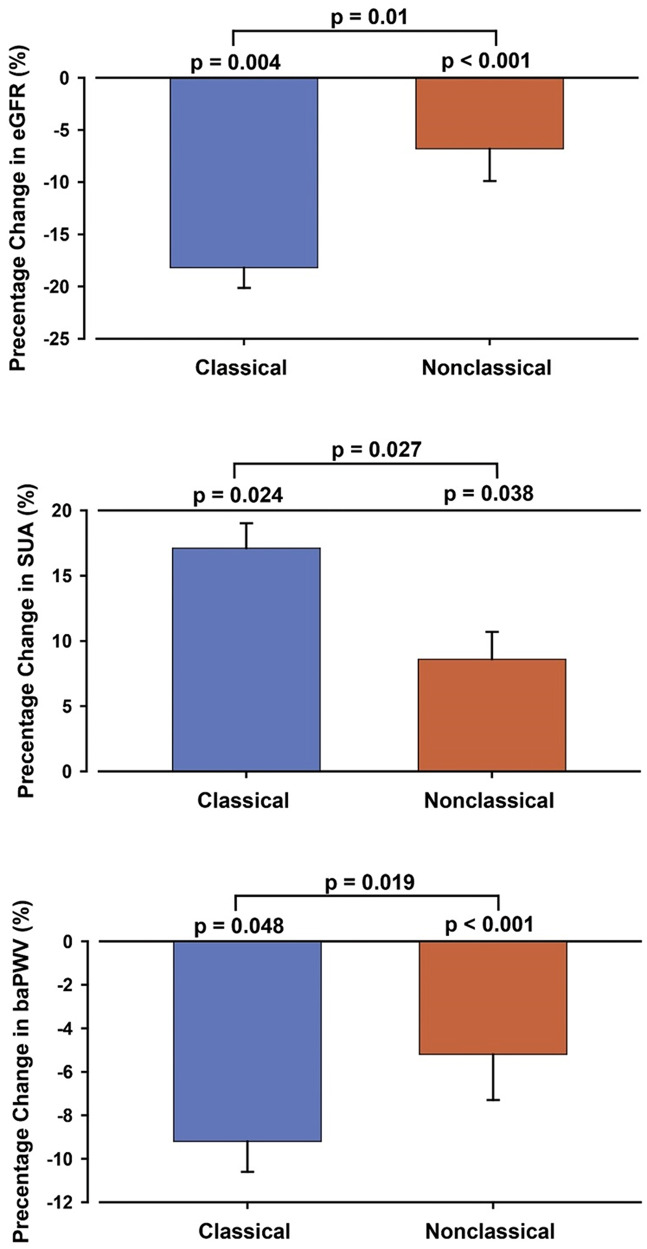
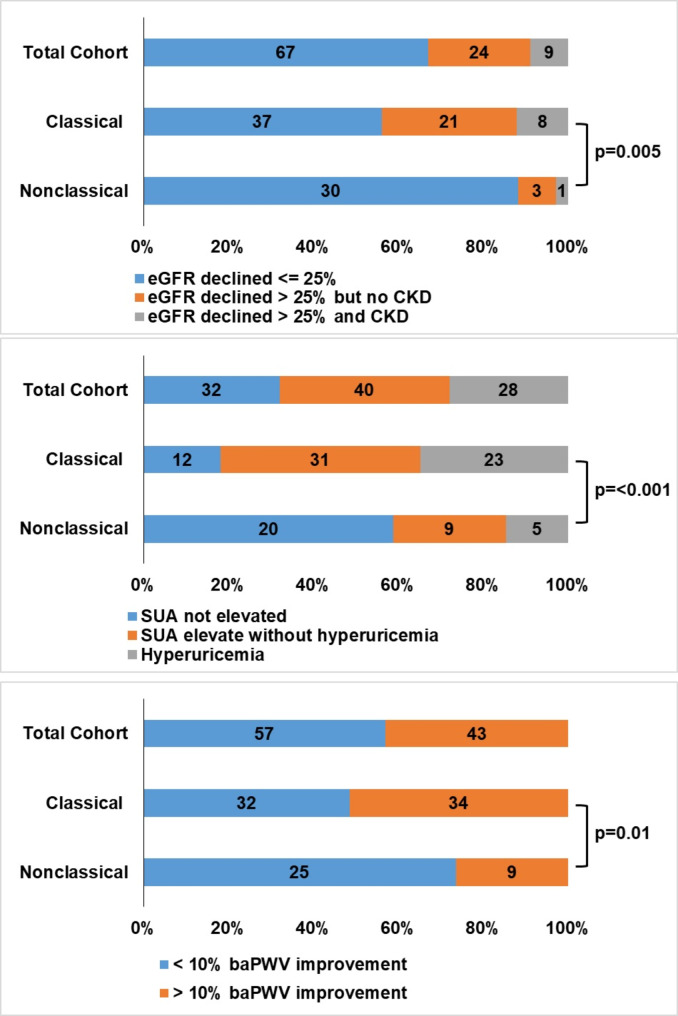
Results: At follow-up, elevated SUA, hyperuricemia, and a > 25% eGFR decrease were significantly more common in the classical than the nonclassical group. The incidence of postoperative hyperuricemia, herein referred to as post-adrenalectomy hyperuricemia (PAHU), was 29% (29/100) overall, 34.8% (23/66) in the classical group and 17.6% (6/34) in the nonclassical group. The incidence of eGFR reduction > 25% was 33% (33/100), 43.9% (29/66), and 11.8% (4/34), respectively. baPWV decreased more in the classical group than the nonclassical group.
Conclusion: For PA patients with PAHU and/or renal impairment, we suggest monitoring SUA, pH, urine uric acid, and urine crystals and performing a KUB study and peripheral vascular and renal sonography (on which pure uric acid stones in the KUB are radiolucent) to determine whether drug intervention is required for cases of asymptomatic PAHU, especially patients in male gender, classical histopathology, or renal impairment.
Keywords: Adrenalectomy; Hyperuricemia; Primary aldosteronism; Renal impairment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Mazza E, Papotti M, Durando R, Robecchi A, Camanni F. Ectopic aldosteronoma associated to another adrenocortical adenoma in the adrenal gland of the same side. J Endocrinol Invest. 1995;18(10):809–12. - PubMed
-
- Williams TA, Gomez-Sanchez CE, Rainey WE, Giordano TJ, Lam AK, Marker A, Mete O, Yamazaki Y, Zerbini MCN, Beuschlein F, Satoh F, Burrello J, Schneider H, Lenders JWM, Mulatero P, Castellano I, Knösel T, Papotti M, Saeger W, Sasano H, Reincke M. International Histopathology Consensus for Unilateral Primary Aldosteronism. J Clin Endocrinol Metab. 2021;106(1):42–54. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
