

HEV ORF2 protein-antibody complex deposits are associated with glomerulonephritis in hepatitis E with reduced immune status
- PMID: 39397005
- PMCID: PMC11471813
- DOI: 10.1038/s41467-024-53072-0
HEV ORF2 protein-antibody complex deposits are associated with glomerulonephritis in hepatitis E with reduced immune status
Abstract
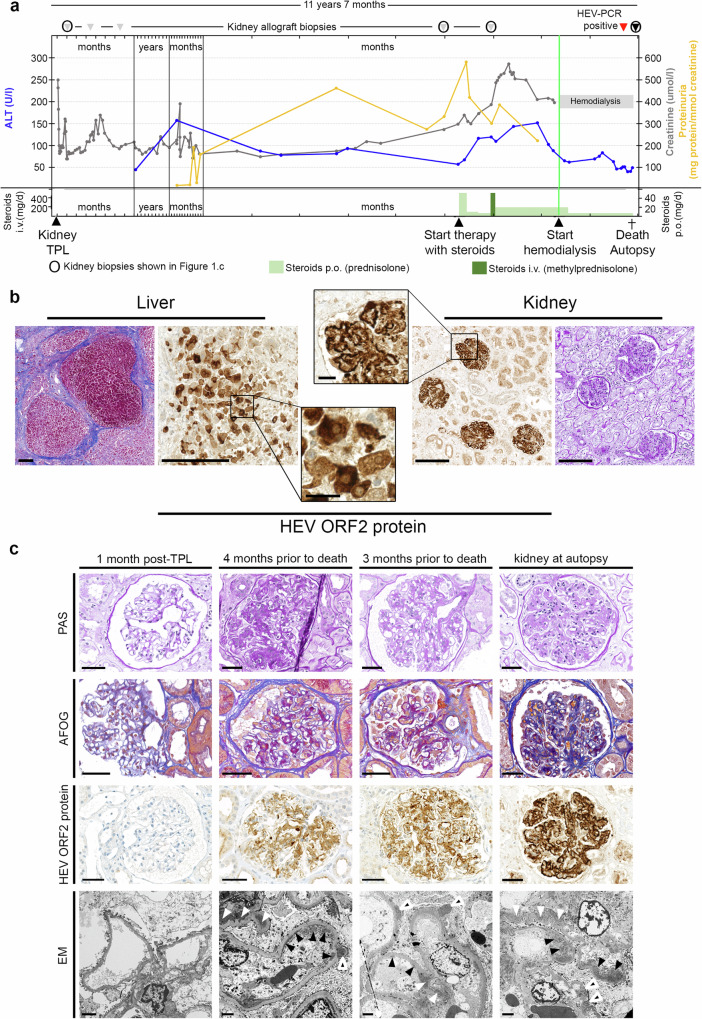
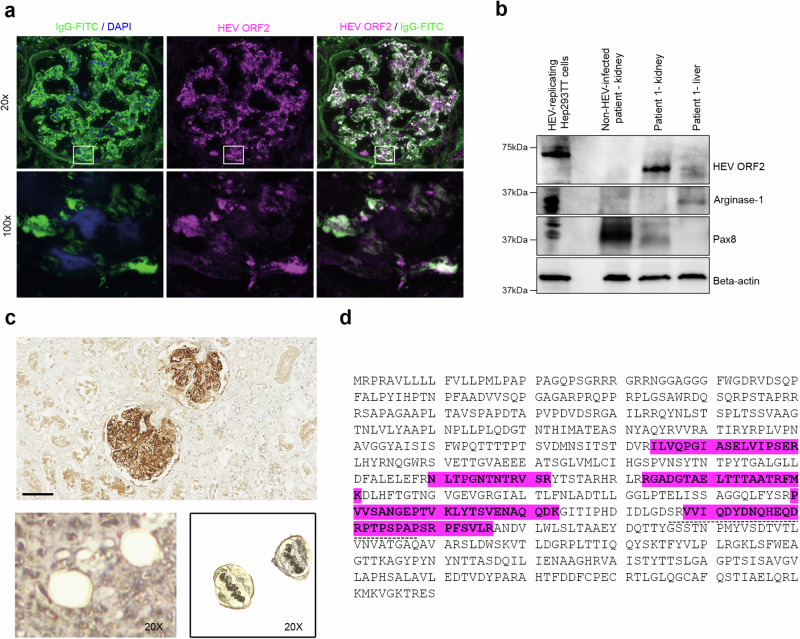
Hepatitis E virus (HEV) infection, one of the most common forms of hepatitis worldwide, is often associated with extrahepatic, particularly renal, manifestations. However, the underlying mechanisms are incompletely understood. Here, we report the development of a de novo immune complex-mediated glomerulonephritis (GN) in a kidney transplant recipient with chronic hepatitis E. Applying immunostaining, electron microscopy, and mass spectrometry after laser-capture microdissection, we show that GN develops in parallel with increasing glomerular deposition of a non-infectious, genome-free and non-glycosylated HEV open reading frame 2 (ORF2) capsid protein. No productive HEV infection of kidney cells is detected. Patients with acute hepatitis E display similar but less pronounced deposits. Our results establish a link between the production of HEV ORF2 protein and the development of hepatitis E-associated GN in the immunocompromised state. The formation of glomerular IgG-HEV ORF2 immune complexes discovered here provides a potential mechanistic explanation of how the hepatotropic HEV can cause variable renal manifestations. These findings directly provide a tool for etiology-based diagnosis of hepatitis E-associated GN as a distinct entity and suggest therapeutic implications.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interest.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
- CRSK-3_190706/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- 310030_207477/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- USZ Innovations-Pool/UniversitätsSpital Zürich (University Hospital Zurich)
LinkOut - more resources
Full Text Sources
