

This is a preprint.
Chronic Low Back Pain Causal Risk Factors Identified by Mendelian Randomization: a Cross-Sectional Cohort Analysis
- PMID: 39399002
- PMCID: PMC11469358
- DOI: 10.1101/2024.09.23.24314235
Chronic Low Back Pain Causal Risk Factors Identified by Mendelian Randomization: a Cross-Sectional Cohort Analysis
Update in
-
Chronic low back pain causal risk factors identified by Mendelian randomization: a cross-sectional cohort analysis.Spine J. 2025 Jun;25(6):1154-1166. doi: 10.1016/j.spinee.2024.12.029. Epub 2025 Jan 14. Spine J. 2025. PMID: 39818276
Abstract
Background context: There are a number of risk factors- from biological, psychological, and social domains- for non-specific chronic low back pain (cLBP). Many cLBP treatments target risk factors on the assumption that the targeted factor is not just associated with cLBP but is also a cause (i.e, a causal risk factor). In most cases this is a strong assumption, primarily due to the possibility of confounding variables. False assumptions about the causal relationships between risk factors and cLBP likely contribute to the generally marginal results from cLBP treatments.
Purpose: The objectives of this study were to a) using rigorous confounding control compare associations between modifiable causal risk factors identified by Mendelian randomization (MR) studies with associations in a cLBP population and b) estimate the association of these risk factors with cLBP outcomes.
Study design/setting: Cross sectional analysis of a longitudinal, online, observational study.
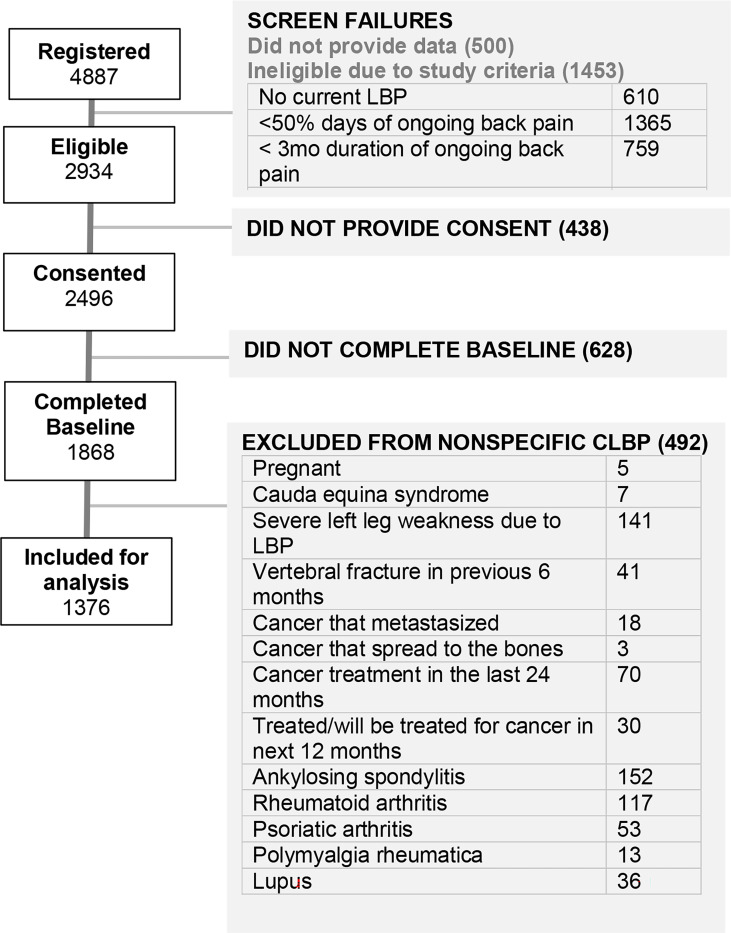
Patient sample: 1,376 participants in BACKHOME, a longitudinal observational e-Cohort of U.S. adults with cLBP that is part of the NIH Back Pain Consortium (BACPAC) Research Program.
Outcome measures: Pain, Enjoyment of Life, and General Activity (PEG) Scale.
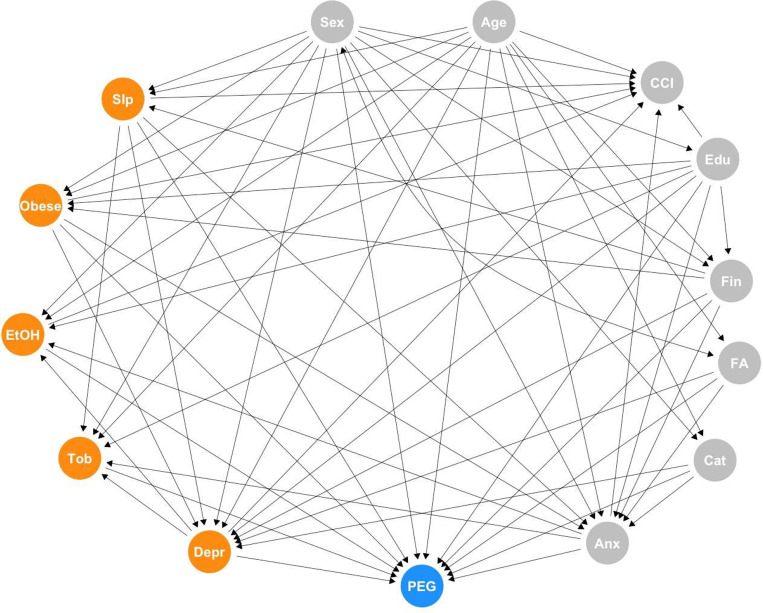
Methods: Five risk factors were selected based on evidence from MR randomization studies: sleep disturbance, depression, BMI, alcohol use, and smoking status. Confounders were identified using the ESC-DAG approach, a rigorous method for building directed acyclic graphs based on causal criteria. Strong evidence for confounding was found for age, female sex, education, relationship status, financial strain, anxiety, fear avoidance and catastrophizing. These variables were used to determine the adjustment sets for the primary analysis. Potential confounders with weaker evidence were used for a sensitivity analysis.
Results: Participants had the following characteristics: age 54.9 ± 14.4 years, 67.4% female, 60% never smokers, 29.9% overweight, 39.5% obese, PROMIS sleep disturbance T-score 54.8 ± 8.0, PROMIS depression T-score 52.6 ± 10.1, Fear-avoidance Beliefs Questionnaire 11.6 ± 5.9, Patient Catastrophizing Scale 4.5 ± 2.6, PEG 4.4 ± 2.2. In the adjusted models alcohol use, sleep disturbance, depression, and obesity were associated with PEG, after adjusting for confounding variables identified via a DAG constructed using a rigorous protocol. The adjusted effect estimates- the expected change in the PEG outcome for every standard deviation increase or decrease in the exposure (or category shift for categorical exposures) were the largest for sleep disturbance and obesity. Each SD increase in the PROMIS sleep disturbance T-score resulted in a mean 0.77 (95% CI: 0.66, 0.88) point increase in baseline PEG score. Compared to participants with normal BMI, adjusted mean PEG score was slightly higher by 0.37 points (95% CI: 0.09, 0.65) for overweight participants, about 0.8 to 0.9 points higher for those in obesity classes I and II, and 1.39 (95% CI: 0.98, 1.80) points higher for the most obese participants. Each SD increase in the PROMIS depression T-score was associated with a mean 0.28 (95% CI: 0.17, 0.40) point increase in baseline PEG score, while each SD decrease in number of alcoholic drinks per week resulted in a mean 0.12 (95%CI: 0.01, 0.23) increase in baseline PEG score in the adjusted model.
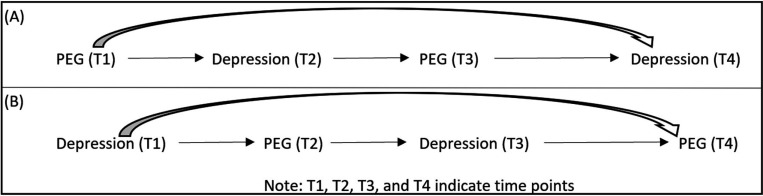
Conclusions: Several modifiable causal risk factors for cLBP - alcohol use, sleep disturbance, depression, and obesity- are associated with PEG, after adjusting for confounding variables identified via a DAG constructed using a rigorous protocol. Convergence of our findings for sleep disturbance, depression, and obesity with the results from MR studies, which have different designs and biases, strengthens the evidence for causal relationships between these risk factors and cLBP (1). The estimated effect of change in a risk factors on change in PEG were the largest for sleep disturbance and obesity. Future analyses will evaluate these relationships with longitudinal data.
Keywords: Epidemiology; Methodology/statistics.
Figures
References
-
- Oliveira CB, Maher CG, Pinto RZ, Traeger AC, Lin CC, Chenot JF, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–803. - PubMed
-
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Annals of Internal Medicine. 2017;166(7):514–30. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources