

Simultaneous Pancreas-Kidney Transplant Outcomes Stratified by Autoantibodies Status and Pretransplant Fasting C-peptide
- PMID: 39399059
- PMCID: PMC11469883
- DOI: 10.1097/TXD.0000000000001721
Simultaneous Pancreas-Kidney Transplant Outcomes Stratified by Autoantibodies Status and Pretransplant Fasting C-peptide
Abstract
Backgrounds: Pancreatic beta cell function and islet autoantibodies classically distinguish types of diabetes (type 1 diabetes mellitus [DM] or type 2 DM). Here, we sought to evaluate simultaneous pancreas-kidney (SPK) transplant outcomes stratified by the presence or absence of beta cell function and autoantibodies.
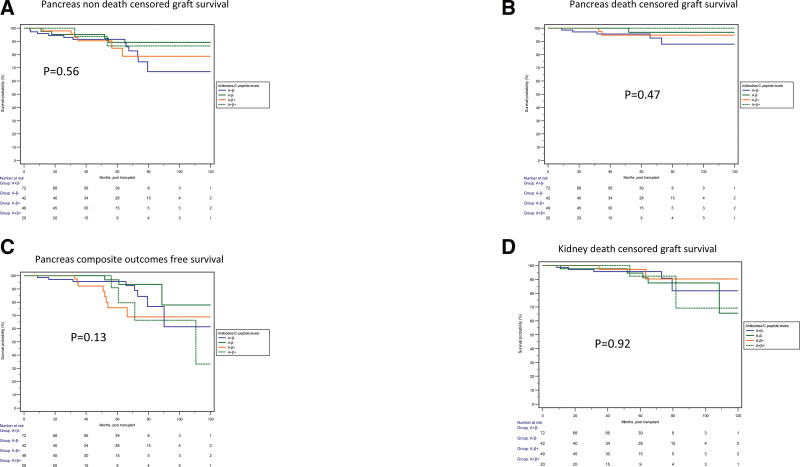
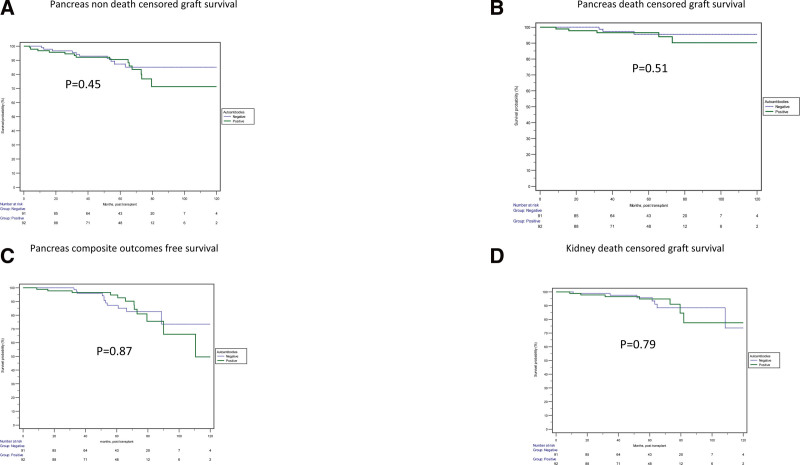
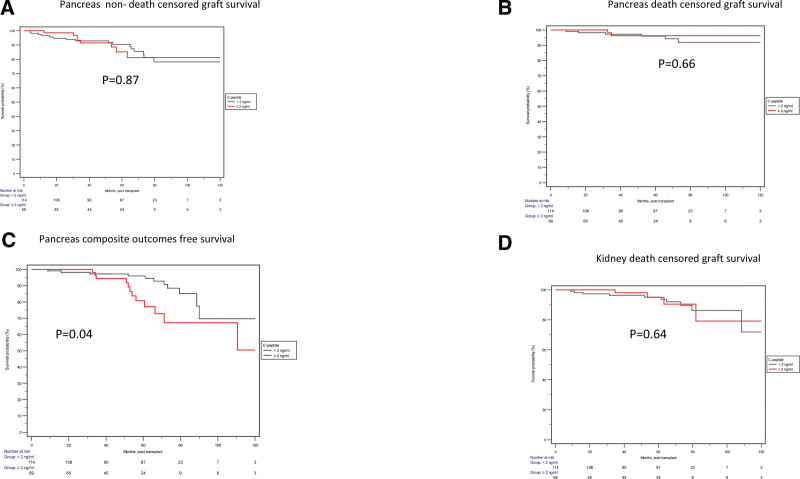
Methods: SPK recipients were eligible if pretransplant autoantibodies were measured against insulin, islet cell, or glutamic acid decarboxylase 65-kD isoform. Recipients were categorized as A+ or A- based on the detection of ≥1 autoantibodies. Recipients were similarly categorized on the basis of detectable pretransplant fasting C-peptide of ≥2 ng/mL (β+) or <2 ng/mL (β-). Thus, recipients were categorized into 4 groups: A+β-, A-β-, A-β+, and A+β+. Outcomes of interest were overall pancreas graft failure (non-death-censored), death-censored pancreas, or kidney graft failure (death-censored pancreas graft failure [DCGF]; kidney DCGF), composite outcomes with any of the 3 outcomes as pancreas DCGF, use of an antidiabetic agent, or hemoglobin A1c >6.5.
Results: One hundred eighty-three SPK recipients were included: A+β- (n = 72), A-β- (n = 42), A-β+ (n = 49), and A+β+ (n = 20). We did not detect a statistical difference in non-death-censored pancreas graft failure for A+β- recipients compared with other groups: A-β- (adjusted hazard ratio [aHR]: 0.44; 95% confidence interval [CI], 0.14-1.42), A-β+ (aHR: 1.02; 95% CI, 0.37-2.85), and A+β+ (aHR: 0.67; 95% CI, 0.13-3.33) in adjusted analyses. Similar outcomes were observed for other outcomes.
Conclusions: In SPK recipients, outcomes were similar among recipients with classic features of type 1 DM and various other types of DM.
Copyright © 2024 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Higher Fasting Pretransplant C-peptide Levels in Type 2 Diabetics Undergoing Simultaneous Pancreas-kidney Transplantation Are Associated With Posttransplant Pancreatic Graft Dysfunction.Transplantation. 2023 Apr 1;107(4):e109-e121. doi: 10.1097/TP.0000000000004489. Epub 2023 Jan 5. Transplantation. 2023. PMID: 36706060 Review.
-
Risk Factors for Early Post-transplant Weight Changes Among Simultaneous Pancreas-kidney Recipients and Impact on Outcomes.Transplant Direct. 2024 Oct 18;10(11):e1720. doi: 10.1097/TXD.0000000000001720. eCollection 2024 Nov. Transplant Direct. 2024. PMID: 39440200 Free PMC article.
-
Kidney Delayed Graft Function in Simultaneous Pancreas-Kidney Transplant Recipients Is Associated With Inferior Outcomes.Transplant Direct. 2025 Apr 17;11(5):e1797. doi: 10.1097/TXD.0000000000001797. eCollection 2025 May. Transplant Direct. 2025. PMID: 40256683 Free PMC article.
-
Outcomes of simultaneous pancreas and kidney transplants based on preemptive transplant compared to those who were on dialysis before transplant - a retrospective study.Transpl Int. 2020 Sep;33(9):1106-1115. doi: 10.1111/tri.13665. Epub 2020 Jun 18. Transpl Int. 2020. PMID: 32479673
-
Lessons learned from more than 1,000 pancreas transplants at a single institution.Ann Surg. 2001 Apr;233(4):463-501. doi: 10.1097/00000658-200104000-00003. Ann Surg. 2001. PMID: 11303130 Free PMC article. Review.
References
-
- 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care. 2020;43(Suppl 1):S14–S31. doi:10.2337/dc21-S002 - PubMed
-
- Törn C. C-peptide and autoimmune markers in diabetes. Clin Lab. 2003;49:1–10. - PubMed
-
- Canivell S, Gomis R. Diagnosis and classification of autoimmune diabetes mellitus. Autoimmun Rev. 2014;13:403–407. - PubMed
LinkOut - more resources
Full Text Sources
