

Development of prognostic models for advanced multiple hepatocellular carcinoma based on Cox regression, deep learning and machine learning algorithms
- PMID: 39399114
- PMCID: PMC11466773
- DOI: 10.3389/fmed.2024.1452188
Development of prognostic models for advanced multiple hepatocellular carcinoma based on Cox regression, deep learning and machine learning algorithms
Abstract
Background: Most patients with multiple hepatocellular carcinoma (MHCC) are at advanced stage once diagnosed, so that clinical treatment and decision-making are quite tricky. The AJCC-TNM system cannot accurately determine prognosis, our study aimed to identify prognostic factors for MHCC and to develop a prognostic model to quantify the risk and survival probability of patients.
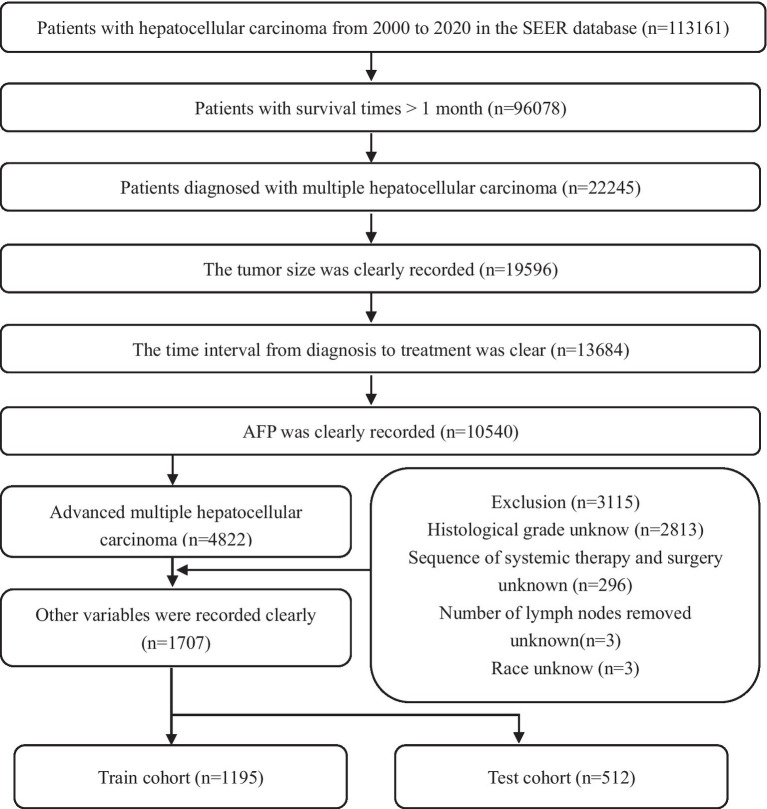
Methods: Eligible patients with HCC were obtained from the Surveillance, Epidemiology, and End Results (SEER) database, and then prognostic models were built using Cox regression, machine learning (ML), and deep learning (DL) algorithms. The model's performance was evaluated using C-index, receiver operating characteristic curve, Brier score and decision curve analysis, respectively, and the best model was interpreted using SHapley additive explanations (SHAP) interpretability technique.
Results: A total of eight variables were included in the follow-up study, our analysis identified that the gradient boosted machine (GBM) model was the best prognostic model for advanced MHCC. In particular, the GBM model in the training cohort had a C-index of 0.73, a Brier score of 0.124, with area under the curve (AUC) values above 0.78 at the first, third, and fifth year. Importantly, the model also performed well in test cohort. The Kaplan-Meier (K-M) survival analysis demonstrated that the newly developed risk stratification system could well differentiate the prognosis of patients.
Conclusion: Of the ML models, GBM model could predict the prognosis of advanced MHCC patients most accurately.
Keywords: advanced multiple hepatocellular carcinoma; deep learning; gradient boosted machine; machine learning; prognosis.
Copyright © 2024 Shen, Zhou, Pei, Yang, Zhao and Ding.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
Deep learning models for predicting the survival of patients with hepatocellular carcinoma based on a surveillance, epidemiology, and end results (SEER) database analysis.Sci Rep. 2024 Jun 9;14(1):13232. doi: 10.1038/s41598-024-63531-9. Sci Rep. 2024. PMID: 38853169 Free PMC article.
-
Construction and validation of a nomogram for patients with multiple hepatocellular carcinoma: A SEER-based study.Eur J Surg Oncol. 2023 Oct;49(10):106966. doi: 10.1016/j.ejso.2023.06.018. Epub 2023 Jun 21. Eur J Surg Oncol. 2023. PMID: 37365056
-
Automated machine learning for predicting liver metastasis in patients with gastrointestinal stromal tumor: a SEER-based analysis.Sci Rep. 2024 May 30;14(1):12415. doi: 10.1038/s41598-024-62311-9. Sci Rep. 2024. PMID: 38816560 Free PMC article.
-
The development of a prediction model based on deep learning for prognosis prediction of gastrointestinal stromal tumor: a SEER-based study.Sci Rep. 2024 Mar 19;14(1):6609. doi: 10.1038/s41598-024-56701-2. Sci Rep. 2024. PMID: 38504089 Free PMC article.
-
Prognosis prediction and risk stratification of transarterial chemoembolization or intraarterial chemotherapy for unresectable hepatocellular carcinoma based on machine learning.Eur Radiol. 2024 Aug;34(8):5094-5107. doi: 10.1007/s00330-024-10581-2. Epub 2024 Jan 30. Eur Radiol. 2024. PMID: 38291256 Free PMC article.
Cited by
-
Integrating radiomics and machine learning for the diagnosis and prognosis of hepatocellular carcinoma.World J Gastrointest Oncol. 2025 Jul 15;17(7):106610. doi: 10.4251/wjgo.v17.i7.106610. World J Gastrointest Oncol. 2025. PMID: 40697211 Free PMC article.
References
LinkOut - more resources
Full Text Sources