

Three-Year Overall Survival Outcomes and Correlative Analyses in Patients With NSCLC and High (50%-89%) Versus Very High (≥90%) Programmed Death-Ligand 1 Expression Treated With First-Line Pembrolizumab or Cemiplimab
- PMID: 39399157
- PMCID: PMC11471150
- DOI: 10.1016/j.jtocrr.2024.100675
Three-Year Overall Survival Outcomes and Correlative Analyses in Patients With NSCLC and High (50%-89%) Versus Very High (≥90%) Programmed Death-Ligand 1 Expression Treated With First-Line Pembrolizumab or Cemiplimab
Abstract
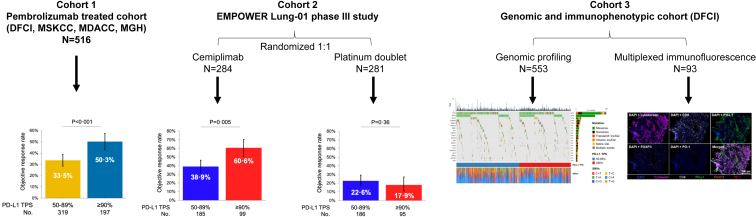
Introduction: Responses to first-line programmed cell death protein 1 inhibition vary among patients with metastatic NSCLC and a programmed death-ligand 1 (PD-L1) tumor proportion score (TPS) greater than or equal to 50%. We previously reported improved clinical outcomes to first-line programmed cell death protein 1 inhibition in patients with metastatic NSCLC with a PD-L1 TPS of greater than or equal to 90% versus 50% to 89% in a pilot study. Here, we report the three-year survival with first-line pembrolizumab and cemiplimab in two large independent cohorts of patients with PD-L1 TPS greater than or equal to 90% versus 50% to 89% and characterize genomic and immunophenotypic differences between these PD-L1 expression groups, which were largely unknown.
Methods: We analyzed three-year outcomes of the following two independent cohorts: (1) a multicenter cohort of patients from four academic centers in the United States treated with pembrolizumab and (2) EMPOWER-Lung 1, randomized, phase III trial comparing first-line cemiplimab with chemotherapy. Tumor genomic profiling and multiplexed immunofluorescence were performed to evaluate genomic and immunophenotypic correlates of very high PD-L1 expression.
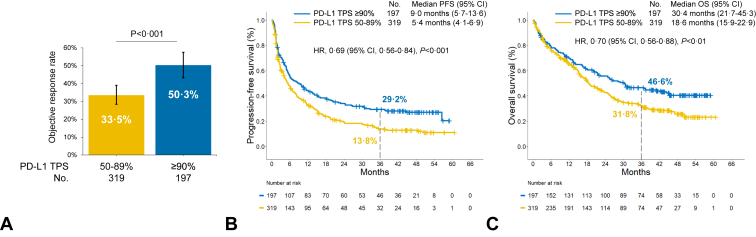
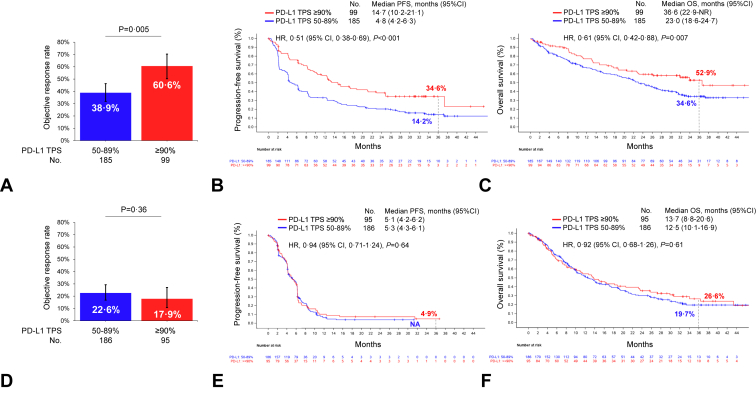
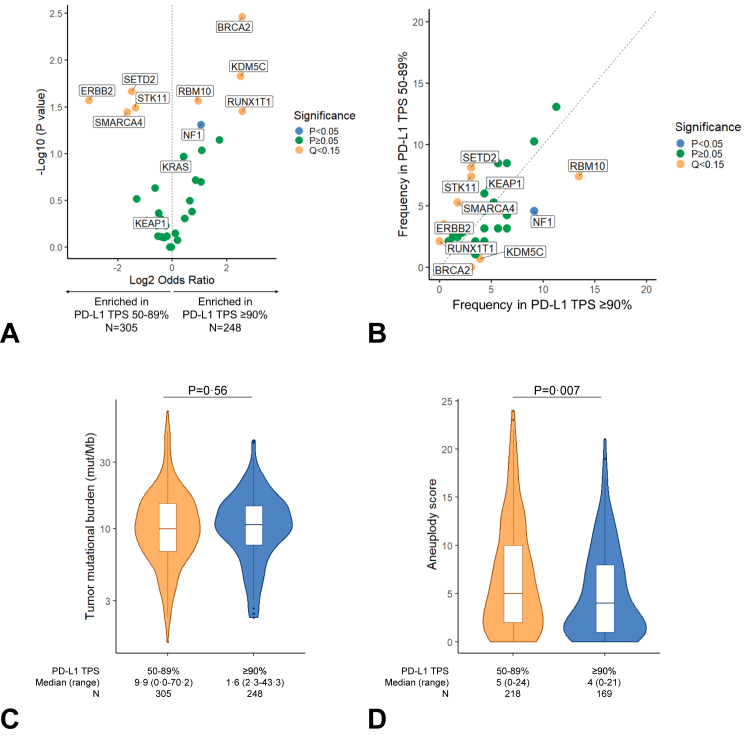
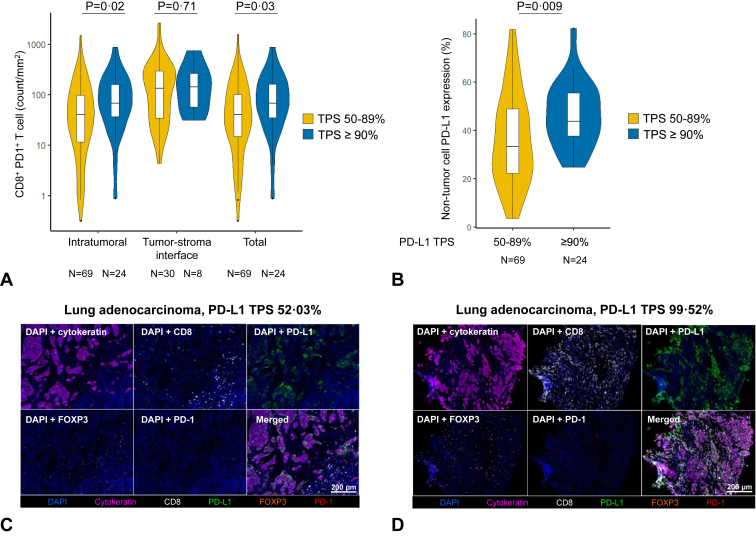
Results: At three years of follow-up, progression-free survival (hazard ratio [HR], 0.69; p < 0.001) and overall survival (HR, 0.70; p < 0.01) to first-line commercial pembrolizumab were significantly improved in patients with a PD-L1 TPS greater than or equal to 90% versus 50% to 89%. In the EMPOWER-Lung 1, patients assigned to the cemiplimab arm with a PD-L1 TPS greater than or equal to 90% also had significant improvements in progression-free survival (HR, 0.53; p < 0.0001) and overall survival (HR, 0.63; p = 0.007) compared with those with a PD-L1 of 50% to 89%. Tumor genomic profiling of 553 NSCLC samples revealed that mutations in STK11 and SMARCA4 were significantly more frequent in tumors with a PD-L1 TPS of 50% to 89% compared with those with a PD-L1 TPS greater than or equal to 90% (Q < 0.15), whereas BRCA2 was enriched in NSCLC samples with a PD-L1 TPS greater than or equal to 90% (Q < 0.15). Multiplexed immunofluorescence on 93 NSCLC samples identified higher intratumoral CD8+PD1+ T cells (p = 0.02) in tumors with PD-L1 TPS greater than or equal to 90% versus 50% to 89%.
Conclusion: Pembrolizumab and cemiplimab were found to have long-term survival benefit and favorable genomic and immunophenotypic profile in patients with advanced NSCLC with PD-L1 TPS greater than or equal to 90% compared with TPS 50% to 89%.
Keywords: Biomarkers; Cemiplimab; Long-term outcomes; PD-L1; Pembrolizumab.
© 2024 The Authors.
Conflict of interest statement
Dr. Ricciuti reports serving on the consulting/advisory board of AstraZeneca, Amgen, and Regeneron; receiving honoraria from Targeted Oncology; and receiving speaker fees from AstraZeneca. Dr. Lin reports receiving consulting from Genentech, C4 Therapeutics, Blueprint Medicines, Nuvalent, Bayer, Elevation Oncology, Novartis, Mirati Therapeutics, Regeneron, Pfizer, Takeda, Ellipses Pharma, Hyku BioSciences, AnHeart Therapeutics, Claim Therapeutics, Turning Point Therapeutics, Bristol-Myers Squibb, and Daiichi Sankyo; receiving institutional research funding from Hengrui Therapeutics, Turning Point Therapeutics, Neon Therapeutics, 10.13039/100019393Relay Therapeutics, 10.13039/100004326Bayer, Elevation Oncology, 10.13039/100004337Roche, Linnaeus Therapeutics, Nuvalent, and 10.13039/100004336Novartis. Dr. Altan reports receiving research funding (to institution) from Genentech, Nektar Therapeutics, Merck, GlaxoSmithKline, Novartis, Jounce Therapeutics, Bristol-Myers Squibb, Eli Lilly, Adaptimmune, Shattuck Lab, and Gilead; serving on the advisory board of GlaxoSmithKline, Shattuck Lab, Bristol-Myers Squibb, AstraZeneca, and Insightec; receiving speaker fees from AstraZeneca, Nektar Therapeutics, and SITC; and having participation of safety review committee for Nanobiotix-MDA Alliance and Hengenix. Dr. Zhang reports receiving grants from 10.13039/100004334Merck; grants and personal fees from Johnson and Johnson and Novartis; and personal fees from Bristol-Myers Squibb, AstraZeneca, GenePlus, Innovent, Varian, Catalyst, and Hengrui, outside the submitted work. Dr. Gainor has served as a compensated consultant or received honoraria from Bristol-Myers Squibb, Genentech/Roche, Takeda, Loxo/Lilly, Blueprint Medicine, Gilead, Moderna, AstraZeneca, Mariana Therapeutics, Mirati, Jounce, Merus Pharmaceuticals, Nuvalent, Pfizer, Novocure, AI Proteins, Novartis, Merck, iTeos, Karyopharm, and Silverback Therapeutics; has received research support from 10.13039/100004336Novartis, Genentech/Roche, and Takeda; has received institutional research support from 10.13039/100002491Bristol-Myers Squibb, Palleon, Tesaro, 10.13039/100019533Moderna, Blueprint, Jounce, 10.13039/100007174Array Biopharma, Merck, Adaptimmune, Novartis, and Alexo; has equity in AI Proteins; and has an immediate family member who is an employee with equity at Ironwood Pharmaceuticals. Dr. Heymach reports serving on the advisory committees of Genentech, Mirati Therapeutics, Eli Lilly & Co., Janssen Pharmaceuticals, Boehringer-Ingelheim Pharmaceuticals, Regeneron, Takeda Pharmaceuticals, BerGenBio, Jazz Pharmaceuticals, Curio Science, Novartis, AstraZeneca Pharmaceuticals, BioAlta, Sanofi, Spectrum Pharmaceuticals, GlaxoSmithKline, EMD Serono, BluePrint Medicine, and Chugai Pharmaceutical; receiving research support from 10.13039/100004325AstraZeneca, Boehringer-Ingelheim, 10.13039/100006399Spectrum, Mirati, Bristol-Myers Squibb, and Takeda; and receiving licensing/royalties from Spectrum. Dr. Pouliot reports being an employee at Regeneron and a Regeneron shareholder. Dr. McIntyre reports being an employee at Regeneron. Dr. Awad reports receiving research funding from Bristol-Myers Squibb, Lilly, 10.13039/100004328Genentech, AstraZeneca, and Elva J. and Clayton L. McLaughlin Fund for Lung Cancer Research; receiving consulting fees from/serving on the advisory board of Merck, Bristol-Myers Squibb, Genentech, AstraZeneca, Nektar, Maverick, Blueprint Medicine, Syndax, AbbVie, Gritstone, ArcherDX, Mirati, NextCure, and EMD Serono. Dr. Rietschel reports being an employee at Regeneron and a Regeneron shareholder with patent issued PCT/US2018/018747. Dr. Nishino reports receiving research funding from Merck, Canon Medical Systems, AstraZeneca, and 10.13039/501100022274Daiichi Sankyo; receiving consulting fees from Daiichi Sankyo and AstraZeneca; and receiving honoraria from Roche. Dr. Sholl reports receiving consulting fee from Genentech, Lilly, and GV20 Therapeutics. The remaining authors have no conflict of interests to disclose.
Figures
References
-
- Reck M., Rodriguez-Abreu D., Robinson A.G., et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive non-small-Cell Lung Cancer. N Engl J Med. 2016;375:1823–1833. - PubMed
-
- Mok T.S.K., Wu Y.L., Kudaba I., et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393:1819–1830. - PubMed
-
- Herbst R.S., Giaccone G., de Marinis F., et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N Engl J Med. 2020;383:1328–1339. - PubMed
-
- Sezer A., Kilickap S., Gümüş M., et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021;397:592–604. - PubMed
-
- Gandhi L., Rodríguez-Abreu D., Gadgeel S., et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378:2078–2092. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
