

Predictive value of immune-related parameters in severe Mycoplasma pneumoniae pneumonia in children
- PMID: 39399713
- PMCID: PMC11467233
- DOI: 10.21037/tp-24-172
Predictive value of immune-related parameters in severe Mycoplasma pneumoniae pneumonia in children
Abstract
Background: The severity of Mycoplasma pneumoniae pneumonia (MPP) is strongly correlated with the extent of the host's immune-inflammatory response. In order to diagnose the severity of MPP early, this study sought to explore the predictive value of immune-related parameters in severe MPP (sMPP) in admitted children.
Methods: We performed a database analysis consisting of patients diagnosed at our medical centers with MPP between 2021 and 2023. We included pediatric patients and examined the association between complete blood cell count (CBC), lymphocyte subsets and the severity of MPP. Binary logistic regression was performed to identify the independent risk factors of sMPP. Receiver operating characteristic (ROC) curves were used to estimate discriminant ability.
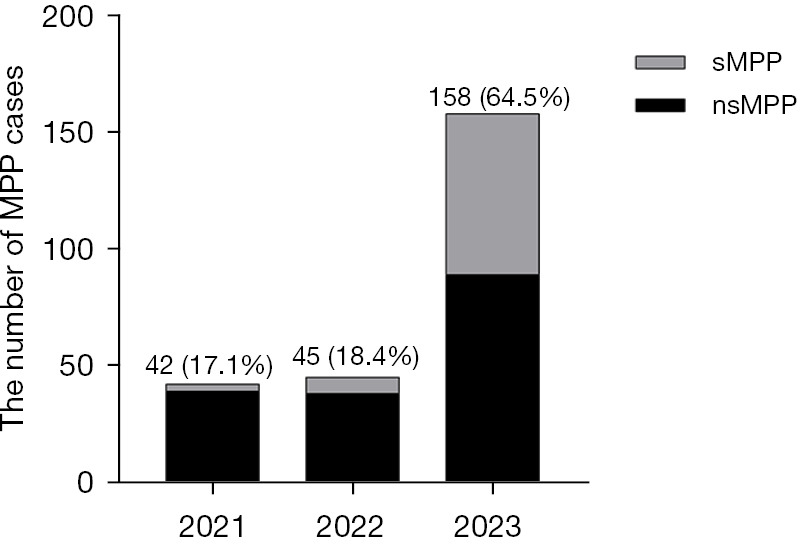
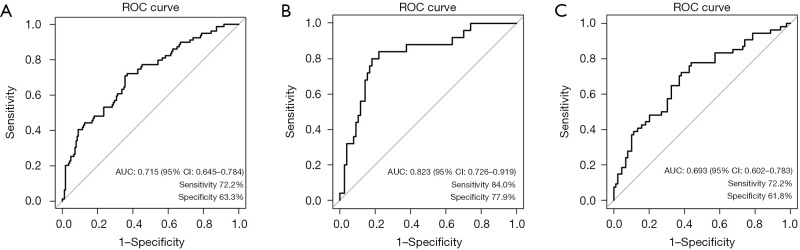
Results: A total of 245 MPP patients were included in the study, with 131 males and 114 females, median aged 6.0 [interquartile range (IQR), 4.0-8.0] years, predominantly located in 2023, and accounted for 64.5%. Among them, 79 pediatric patients were diagnosed as sMPP. The parameters of CBC including white blood cell (WBC) counts, neutrophil counts, monocyte counts, platelet counts, and neutrophil-to-lymphocyte ratio (NLR), were higher in the sMPP group (all P<0.05). The parameters of lymphocyte subsets including CD3+ T cell ratio (CD3+%) and CD3+CD8+ T cell ratio (CD3+CD8+%), were lower in the sMPP group (all P<0.05). And CD3-CD19+ B cell ratio (CD3-CD19+%) was higher in the sMPP group. Logistic regression analysis showed that age, CD3-CD19+%, and monocyte counts were identified as independent risk factors for the development of sMPP (all P<0.001). The three factors were applied in constructing a prediction model that was tested with 0.715 of the area under the ROC curve (AUC). The AUC of the prediction model for children aged ≤5 years was 0.823 and for children aged >5 years was 0.693.
Conclusions: The predictive model formulated by age, CD3-CD19+%, and monocyte counts may play an important role in the early diagnosis of sMPP in admitted children, especially in children aged ≤5 years.
Keywords: Mycoplasma pneumoniae pneumonia (MPP); pediatrics; risk factor; severity prediction.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tp.amegroups.com/article/view/10.21037/tp-24-172/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Predictive value of Ig Mycoplasma pneumoniae-DNA, high-density lipoprotein, natural killer cell, and platelet levels for diagnosing severe M. pneumoniae pneumonia in children.Indian J Med Microbiol. 2025 Jan-Feb;53:100770. doi: 10.1016/j.ijmmb.2024.100770. Epub 2024 Dec 7. Indian J Med Microbiol. 2025. PMID: 39638043
-
The Clinical Value of Systemic Immune Inflammation Index (SII) in Predicting the Severity of Hospitalized Children with Mycoplasma Pneumoniae Pneumonia: A Retrospective Study.Int J Gen Med. 2024 Mar 12;17:935-942. doi: 10.2147/IJGM.S451466. eCollection 2024. Int J Gen Med. 2024. PMID: 38495920 Free PMC article.
-
Clinical characteristics and risk factors for Mycoplasma pneumoniae pneumonia in children.Front Pediatr. 2024 Dec 23;12:1438631. doi: 10.3389/fped.2024.1438631. eCollection 2024. Front Pediatr. 2024. PMID: 39764167 Free PMC article.
-
D-dimer: The Risk Factor of Children's Severe Mycoplasma Pneumoniae Pneumonia.Front Pediatr. 2022 Apr 12;10:828437. doi: 10.3389/fped.2022.828437. eCollection 2022. Front Pediatr. 2022. PMID: 35498793 Free PMC article.
-
[Characteristics of peripheral blood lymphocyte subsets in children with mycoplasma pneumoniae pneumonia under different infection states].Zhonghua Yu Fang Yi Xue Za Zhi. 2025 Mar 6;59(3):344-351. doi: 10.3760/cma.j.cn112150-20240909-00721. Zhonghua Yu Fang Yi Xue Za Zhi. 2025. PMID: 40107785 Chinese.
Cited by
-
Impact of body mass index on clinical outcomes in pediatric patients with mycoplasma pneumoniae pneumonia: a retrospective cohort study.Transl Pediatr. 2025 Apr 30;14(4):608-617. doi: 10.21037/tp-2024-494. Epub 2025 Apr 27. Transl Pediatr. 2025. PMID: 40386353 Free PMC article.
-
Epidemiological characteristics of community-acquired Mycoplasma pneumoniae in hospitalized children around COVID-19 from Jiangsu Province, China: a multicenter retrospective study.Transl Pediatr. 2024 Dec 31;13(12):2155-2163. doi: 10.21037/tp-24-281. Epub 2024 Dec 27. Transl Pediatr. 2024. PMID: 39823007 Free PMC article.
-
Development of machine learning-based differential diagnosis model and risk prediction model of organ damage for severe Mycoplasma pneumoniae pneumonia in children.Sci Rep. 2025 Mar 19;15(1):9431. doi: 10.1038/s41598-025-92089-3. Sci Rep. 2025. PMID: 40108182 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials